Sadan Ofer, Singbartl Kai, Kraft Jacqueline, Plancher Joao McONeil, Greven Alexander C M, Kandiah Prem, Pimentel Cederic, Hall C L, Papangelou Alexander, Asbury William H, Hanfelt John J, Samuels Owen
1Department of Neurology and Neurosurgery, Division of Neurocritical Care, Emory University Hospital and Emory University School of Medicine, 1364 Clifton Rd. NE, Atlanta, GA 30322 USA.
2Department of Critical Care Medicine, Mayo Clinic, 5777 E Mayo Blvd, Phoenix, AZ 85054 USA.
J Intensive Care. 2020 May 4;8:32. doi: 10.1186/s40560-020-00449-0. eCollection 2020.
Recent reports have demonstrated that among patients with subarachnoid hemorrhage (SAH) treated with hypertonic NaCl, resultant hyperchloremia has been associated with the development of acute kidney injury (AKI). We report a trial comparing the effect of two hypertonic solutions with different chloride contents on the resultant serum chloride concentrations in SAH patients, with a primary outcome aimed at limiting chloride elevation.
A low ChloridE hyperTonic solution for brain Edema (ACETatE) trial is a single-center, double-blinded, double-dummy, randomized pilot trial comparing bolus infusions of 23.4% NaCl and 16.4% NaCl/Na-acetate for the treatment of cerebral edema in patients with SAH. Randomization occurred when patients developed hyperchloremia (serum Cl ≥ 109 mmol/L) and required hyperosmolar treatment.
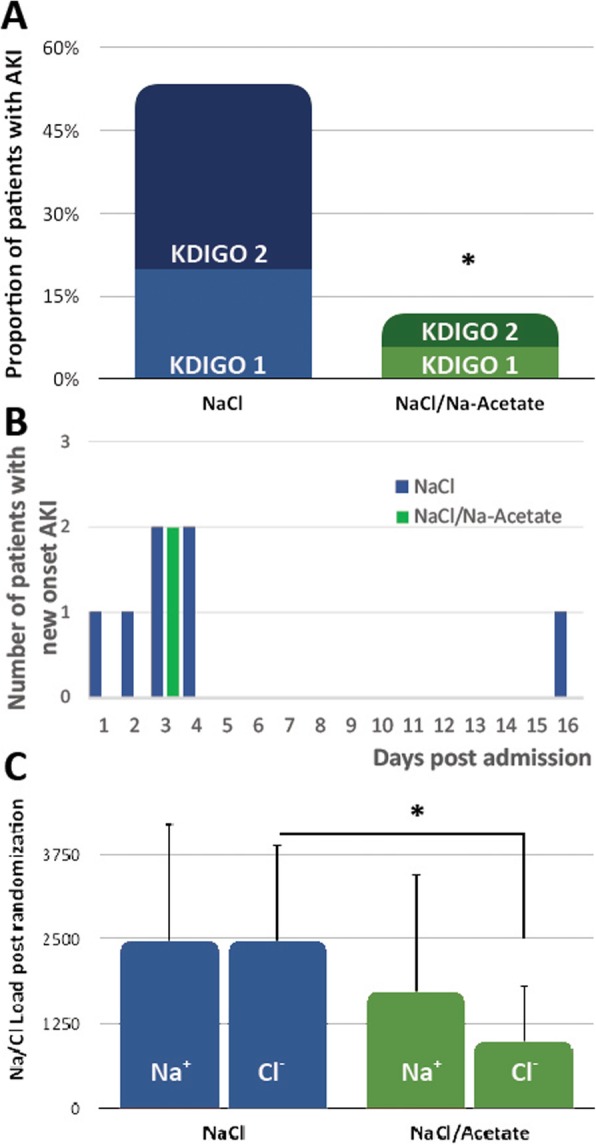
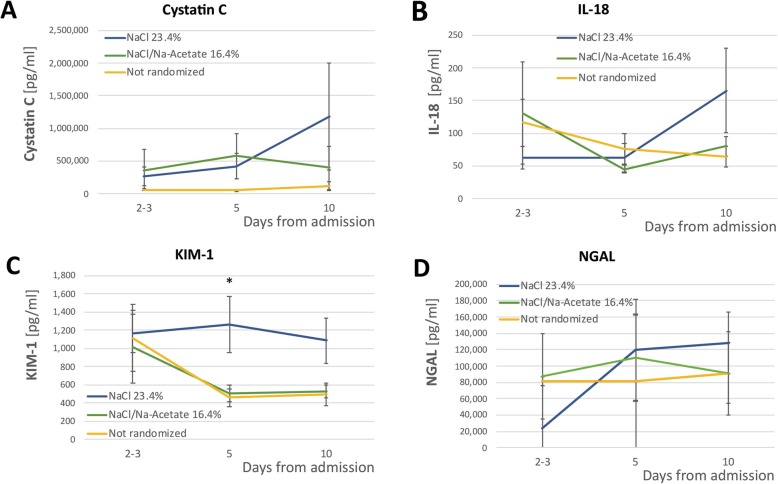
We enrolled 59 patients, of which 32 developed hyperchloremia and required hyperosmolar treatment. 15 patients were randomized to the 23.4% NaCl group, and 17 patients were randomized to the 16.4% NaCl/Na-acetate group. Although serum chloride levels increased similarly in both groups, the NaCl/Acetate group showed a significantly lower Cl load at the end of the study period (978mEq vs. 2,464mEq, < 0.01). Secondary outcome analysis revealed a reduced rate of AKI in the Na-acetate group (53.3% in the NaCl group vs. 11.8% in the Na-acetate group, = 0.01). Both solutions had similar effects on ICP reduction, but NaCl/Acetate treatment had a more prominent effect on immediate post-infusion Na concentrations (increase of 2.2 ± 2.8 vs. 1.4 ± 2.6, ( < 0.01)). Proximal tubule renal biomarkers differed in concentration between the two groups.
Our pilot trial showed the feasibility and safety of replacing 23.4% NaCl infusions with 16.4% NaCl/Na-acetate infusions to treat cerebral edema in patients with SAH. The degree of hyperchloremia was similar in the two groups. 16.4% NaCl/Na-acetate infusions led to lower Cl load and AKI rates than 23.4% NaCl infusions. Further multi-center studies are needed to corroborate these results.
clinicaltrials.gov # NCT03204955, registered on 6/28/2017.
近期报告显示,在接受高渗氯化钠治疗的蛛网膜下腔出血(SAH)患者中,由此导致的高氯血症与急性肾损伤(AKI)的发生有关。我们报告一项试验,比较两种不同氯化物含量的高渗溶液对SAH患者血清氯化物浓度的影响,主要结局旨在限制氯化物升高。
用于脑水肿的低氯高渗溶液(ACETatE)试验是一项单中心、双盲、双模拟、随机试点试验,比较静脉推注23.4%氯化钠和16.4%氯化钠/醋酸钠治疗SAH患者脑水肿的效果。当患者出现高氯血症(血清Cl≥109 mmol/L)并需要高渗治疗时进行随机分组。
我们纳入了59例患者,其中32例出现高氯血症并需要高渗治疗。15例患者被随机分配到23.4%氯化钠组,17例患者被随机分配到16.4%氯化钠/醋酸钠组。虽然两组血清氯化物水平升高相似,但在研究期末,氯化钠/醋酸钠组的Cl负荷显著更低(978mEq对2464mEq,<0.01)。次要结局分析显示醋酸钠组AKI发生率降低(氯化钠组为53.3%,醋酸钠组为11.8%,=0.01)。两种溶液对降低颅内压的效果相似,但氯化钠/醋酸钠治疗对输注后即刻的钠浓度影响更显著(升高2.2±2.8对1.4±2.6,(<0.01))。两组近端肾小管肾生物标志物的浓度有所不同。
我们的试点试验表明,用16.4%氯化钠/醋酸钠输注替代23.4%氯化钠输注治疗SAH患者脑水肿具有可行性和安全性。两组高氯血症程度相似。16.4%氯化钠/醋酸钠输注导致的Cl负荷和AKI发生率低于23.4%氯化钠输注。需要进一步的多中心研究来证实这些结果。
clinicaltrials.gov # NCT03204955,于2017年6月28日注册。