Crouser Elliott D, Parrillo Joseph E, Martin Greg S, Huang David T, Hausfater Pierre, Grigorov Ilya, Careaga Diana, Osborn Tiffany, Hasan Mohamad, Tejidor Liliana
1Division of Pulmonary and Critical Care Medicine, The Ohio State University Wexner Medical Center, 201 Davis Heart & Lung Research Institute, 473 West 12th Avenue, Columbus, OH USA.
2Heart and Vascular Hospital, Hackensack University Medical Center, Hackensack, NJ USA.
J Intensive Care. 2020 May 5;8:33. doi: 10.1186/s40560-020-00446-3. eCollection 2020.
The initial presentation of sepsis in the emergency department (ED) is difficult to distinguish from other acute illnesses based upon similar clinical presentations. A new blood parameter, a measurement of increased monocyte volume distribution width (MDW), may be used in combination with other clinical parameters to improve early sepsis detection. We sought to determine if MDW, when combined with other available clinical parameters at the time of ED presentation, improves the early detection of sepsis.
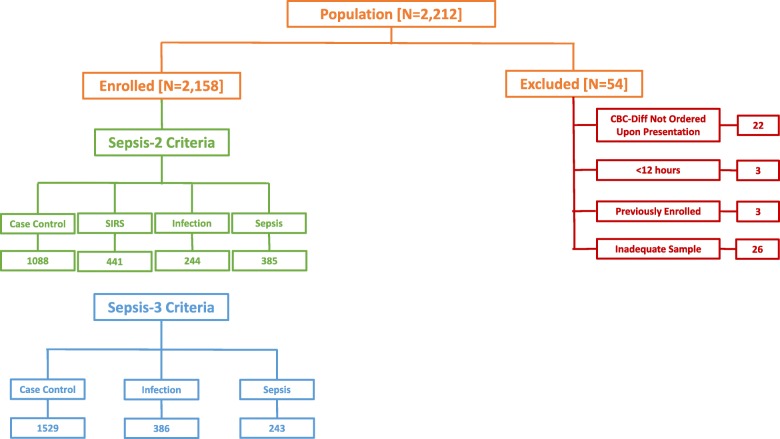
A retrospective analysis of prospectively collected clinical data available during the initial ED encounter of 2158 adult patients who were enrolled from emergency departments of three major academic centers, of which 385 fulfilled Sepsis-2 criteria, and 243 fulfilled Sepsis-3 criteria within 12 h of admission. Sepsis probabilities were determined based on MDW values, alone or in combination with components of systemic inflammatory response syndrome (SIRS) or quick sepsis-related organ failure assessment (qSOFA) score obtained during the initial patient presentation (i.e., within 2 h of ED admission).
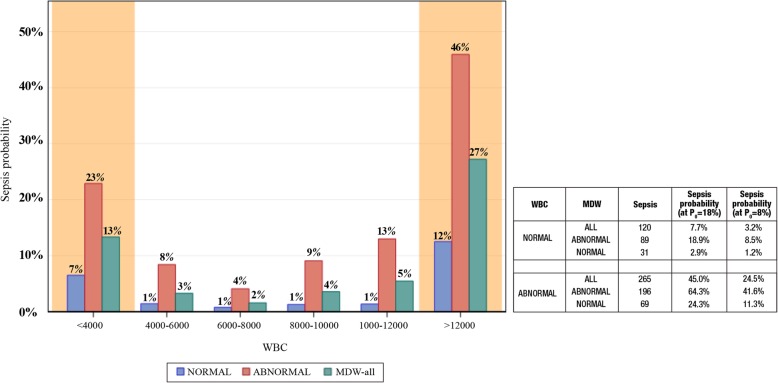
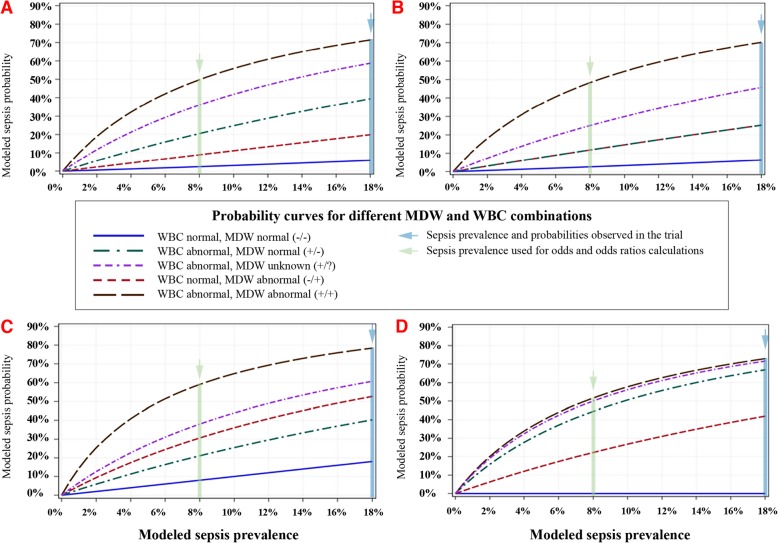
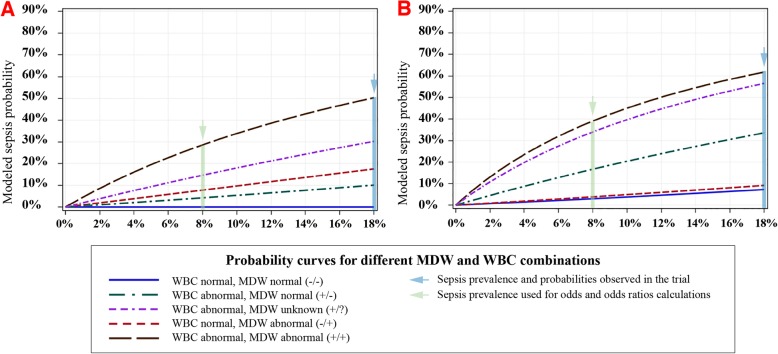
Abnormal MDW (> 20.0) consistently increased sepsis probability, and normal MDW consistently reduced sepsis probability when used in combination with SIRS criteria (tachycardia, tachypnea, abnormal white blood count, or body temperature) or qSOFA criteria (tachypnea, altered mental status, but not hypotension). Overall, and regardless of other SIRS or qSOFA variables, MDW > 20.0 (vs. MDW ≤ 20.0) at the time of the initial ED encounter was associated with an approximately 6-fold increase in the odds of Sepsis-2, and an approximately 4-fold increase in the odds of Sepsis-3.
MDW improves the early detection of sepsis during the initial ED encounter and is complementary to SIRS and qSOFA parameters that are currently used for this purpose. This study supports the incorporation of MDW with other readily available clinical parameters during the initial ED encounter for the early detection of sepsis.
ClinicalTrials.gov, NCT03145428. First posted May 9, 2017. The first subjects were enrolled June 19, 2017, and the study completion date was January 26, 2018.
脓毒症在急诊科的初始表现很难基于相似的临床表现与其他急性疾病区分开来。一种新的血液参数,即单核细胞体积分布宽度(MDW)增加的测量值,可与其他临床参数联合使用以改善脓毒症的早期检测。我们试图确定MDW在与急诊科就诊时其他可用的临床参数联合使用时,是否能改善脓毒症的早期检测。
对前瞻性收集的2158例成年患者在三大医学中心急诊科初始就诊时的临床数据进行回顾性分析,其中385例符合脓毒症-2标准,243例在入院12小时内符合脓毒症-3标准。脓毒症概率根据MDW值单独或与初始患者就诊时(即急诊科入院2小时内)获得的全身炎症反应综合征(SIRS)或快速脓毒症相关器官功能衰竭评估(qSOFA)评分的组成部分联合确定。
异常MDW(>20.0)持续增加脓毒症概率,而正常MDW与SIRS标准(心动过速、呼吸急促、白细胞计数异常或体温)或qSOFA标准(呼吸急促、精神状态改变,但不包括低血压)联合使用时持续降低脓毒症概率。总体而言,无论其他SIRS或qSOFA变量如何,急诊科初始就诊时MDW>20.0(与MDW≤20.0相比)与脓毒症-2几率增加约6倍以及脓毒症-3几率增加约4倍相关。
MDW可改善急诊科初始就诊时脓毒症的早期检测,并且是目前用于此目的的SIRS和qSOFA参数的补充。本研究支持在急诊科初始就诊时将MDW与其他易于获得的临床参数联合用于脓毒症的早期检测。
ClinicalTrials.gov,NCT03145428。首次发布于2017年5月9日。首批受试者于2017年6月19日入组,研究完成日期为2018年1月26日。