Clinical Microbiology and Infectious Diseases, School of Pathology, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa.
Infection Control, Charlotte Maxeke Johannesburg Academic Hospital, National Health Laboratory Service, Johannesburg, South Africa.
PLoS One. 2020 May 11;15(5):e0233102. doi: 10.1371/journal.pone.0233102. eCollection 2020.
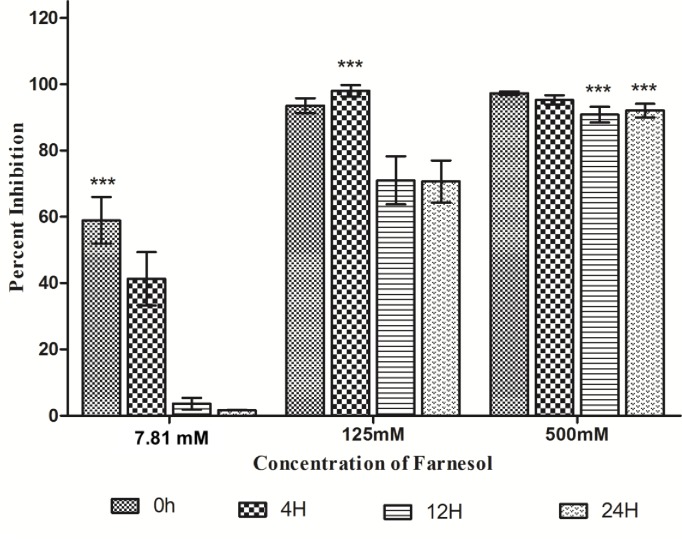
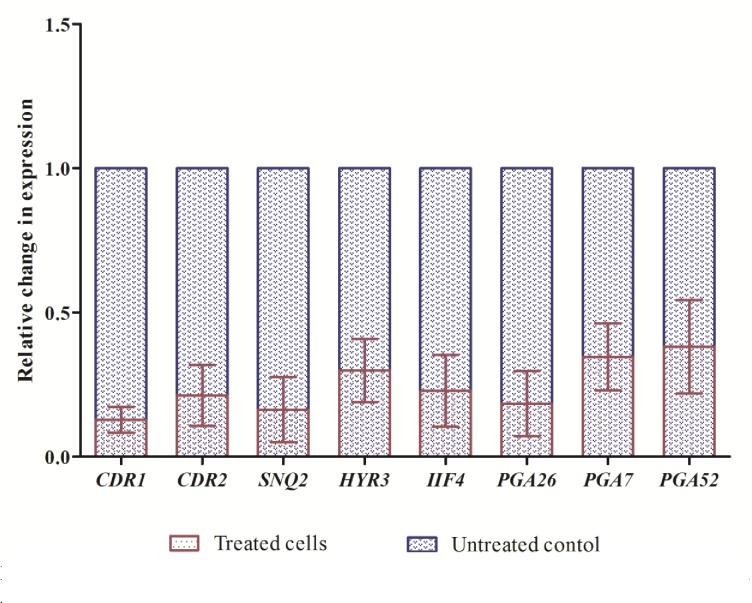
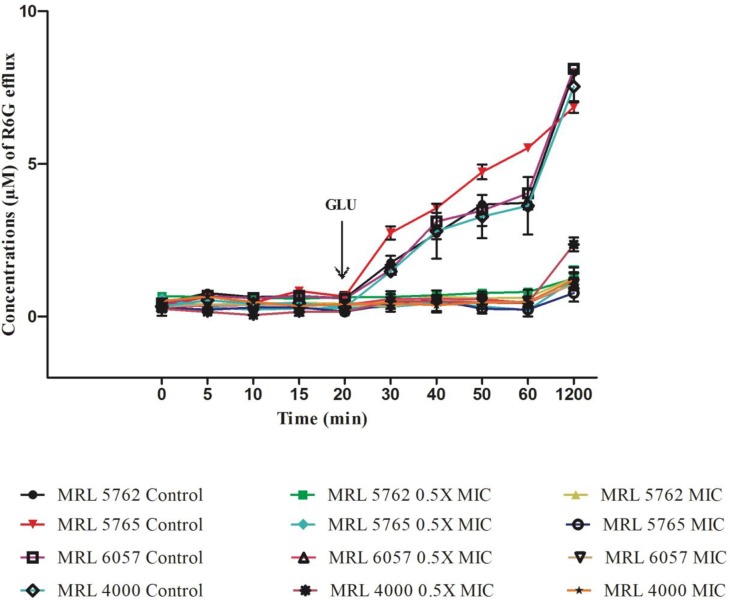
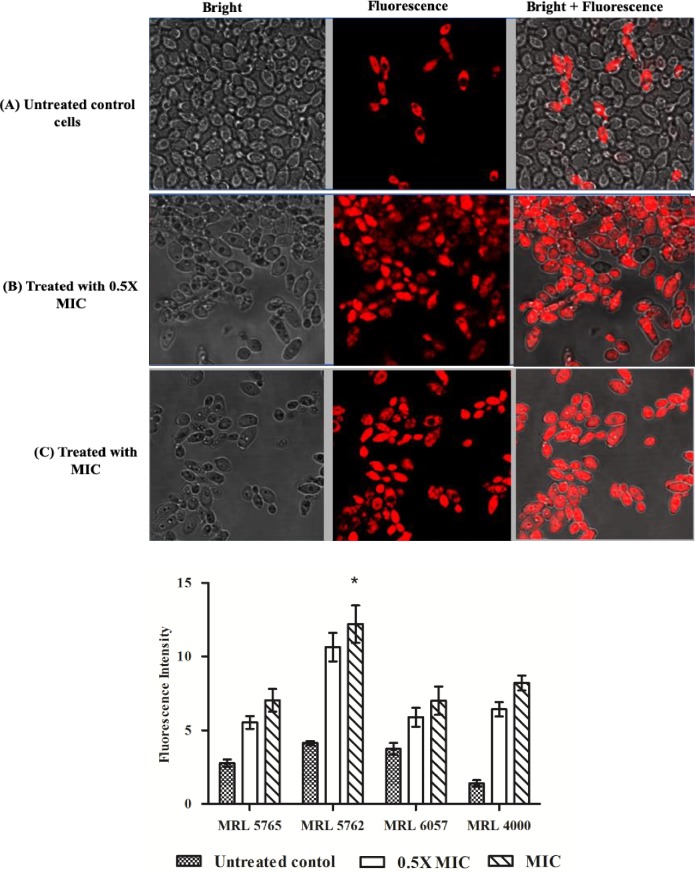
Candida auris, a decade old Candida species, has been identified globally as a significant nosocomial multidrug resistant (MDR) pathogen responsible for causing invasive outbreaks. Biofilms and overexpression of efflux pumps such as Major Facilitator Superfamily and ATP Binding Cassette are known to cause multidrug resistance in Candida species, including C. auris. Therefore, targeting these factors may prove an effective approach to combat MDR in C. auris. In this study, 25 clinical isolates of C. auris from different hospitals of South Africa were used. All the isolates were found capable enough to form biofilms on 96-well flat bottom microtiter plate that was further confirmed by MTT reduction assay. In addition, these strains have active drug efflux mechanism which was supported by rhodamine-6-G extracellular efflux and intracellular accumulation assays. Antifungal susceptibility profile of all the isolates against commonly used drugs was determined following CLSI recommended guidelines. We further studied the role of farnesol, an endogenous quorum sensing molecule, in modulating development of biofilms and drug efflux in C. auris. The MIC for planktonic cells ranged from 62.5-125 mM, and for sessile cells was 125 mM (4h biofilm) and 500 mM (12h and 24h biofilm). Furthermore, farnesol (125 mM) also suppresses adherence and biofilm formation by C. auris. Farnesol inhibited biofilm formation, blocked efflux pumps and downregulated biofilm- and efflux pump- associated genes. Modulation of C. auris biofilm formation and efflux pump activity by farnesol represent a promising approach for controlling life threatening infections caused by this pathogen.
耳念珠菌,一种存在了十年的念珠菌,已在全球范围内被确定为一种重要的医院内多药耐药(MDR)病原体,可导致侵袭性爆发。生物膜和外排泵(如主要易化超家族和 ATP 结合盒)的过度表达,已知会导致念珠菌属,包括耳念珠菌产生多药耐药。因此,针对这些因素可能是对抗耳念珠菌 MDR 的有效方法。在这项研究中,使用了来自南非不同医院的 25 株临床分离的耳念珠菌。所有分离株都有足够的能力在 96 孔平底微量滴定板上形成生物膜,这一点通过 MTT 还原测定进一步得到证实。此外,这些菌株具有活跃的药物外排机制,这得到了罗丹明 6-G 细胞外外排和细胞内积累测定的支持。根据 CLSI 推荐的指南,确定了所有分离株对常用药物的抗真菌药敏谱。我们进一步研究了法尼醇(一种内源性群体感应分子)在调节耳念珠菌生物膜形成和药物外排中的作用。浮游细胞的 MIC 范围为 62.5-125 mM,而 4h 生物膜的固着细胞 MIC 为 125 mM,12h 和 24h 生物膜的 MIC 为 500 mM。此外,法尼醇(125 mM)还抑制耳念珠菌的粘附和生物膜形成。法尼醇抑制生物膜形成,阻断外排泵,并下调生物膜和外排泵相关基因。法尼醇对耳念珠菌生物膜形成和外排泵活性的调节代表了控制这种病原体引起的危及生命感染的一种有前途的方法。