Mel & Enid Zuckerman College of Public Health, University of Arizona, 1295 N. Martin Ave., Tucson, AZ, 85724, USA.
Health Sciences Library, University of Arizona, 1501 N Campbell Ave Ward 6, Tucson, AZ, 85724, USA.
BMC Public Health. 2020 May 11;20(1):654. doi: 10.1186/s12889-020-08777-4.
Sub-Saharan Africa (SSA) experiences disproportionate burden of cervical cancer incidence and mortality due in part to low uptake of cervical screening, a strategy for prevention and down-staging of cervical cancer. This scoping review identifies studies of interventions to increase uptake of cervical screening among women in the region and uses the Integrated Behavioral Model (IBM) to describe how interventions might work.
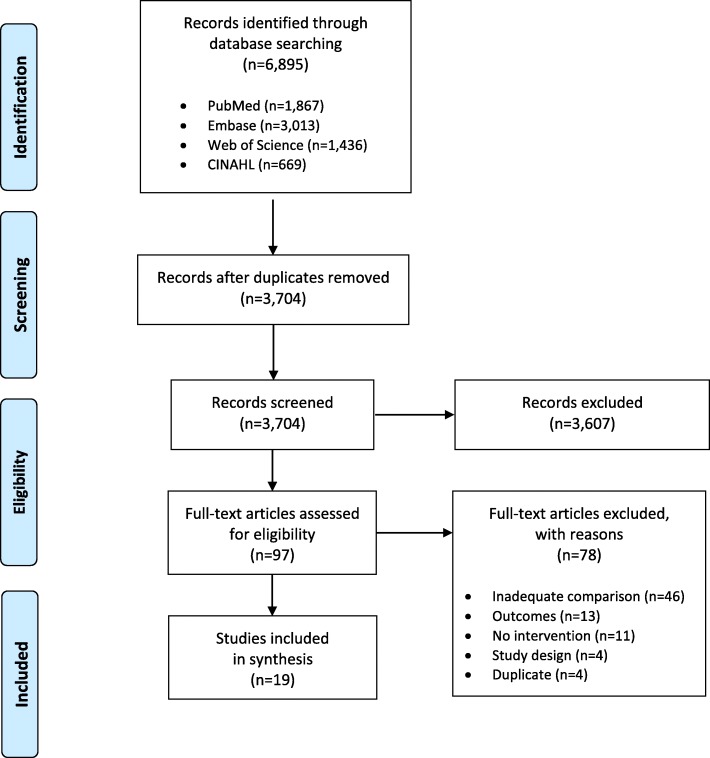
A systematic search of literature was conducted in PubMed, Web of Science, Embase, and CINAHL databases through May 2019. Screening and data charting were performed by two independent reviewers. Intervention studies measuring changes to uptake in screening among women in SSA were included, with no restriction to intervention type, study setting or date, or participant characteristics. Intervention type and implementation strategies were described using behavioral constructs from the IBM.
Of the 3704 citations the search produced, 19 studies were selected for inclusion. Most studies were published between 2014 and 2019 (78.9%) and were set in Nigeria (47.4%) and South Africa (26.3%). Studies most often assessed screening with Pap smears (31.6%) and measured uptake as ever screened (42.1%) or screened during the study period (36.8%). Education-based interventions were most common (57.9%) and the IBM construct of knowledge/skills to perform screening was targeted most frequently (68.4%). Willingness to screen was high, before and after intervention. Screening coverage ranged from 1.7 to 99.2% post-intervention, with six studies (31.6%) reporting a significant improvement in screening that achieved ≥60% coverage.
Educational interventions were largely ineffective, except those that utilized peer or community health educators and mHealth implementation strategies. Two economic incentivization interventions were moderately effective, by acting on participants' instrumental attitudes, but resulted in screening coverage less than 20%. Innovative service delivery, including community-based self-sampling, acted on environmental constraints, striving to make services more available, accessible, and appropriate to women, and were the most effective. This review demonstrates that intent to perform screening may not be the major determinant of screening behavior, suggesting other theoretical frameworks may be needed to more fully understand uptake of cervical screening in sub-Saharan Africa, particularly for health systems change interventions.
撒哈拉以南非洲(SSA)的宫颈癌发病率和死亡率负担不成比例,部分原因是宫颈癌筛查的接受率低,而宫颈癌筛查是预防和降低宫颈癌分期的策略。本范围界定审查确定了旨在增加该地区妇女接受宫颈癌筛查的干预措施的研究,并使用综合行为模型(IBM)来描述干预措施的作用方式。
通过 2019 年 5 月在 PubMed、Web of Science、Embase 和 CINAHL 数据库中进行系统文献检索。由两名独立的审查员进行筛查和数据图表制作。纳入了测量撒哈拉以南非洲妇女筛查接受率变化的干预研究,对干预类型、研究地点或日期或参与者特征没有限制。使用 IBM 的行为结构描述了干预类型和实施策略。
搜索产生的 3704 条引文,有 19 项研究入选。大多数研究发表于 2014 年至 2019 年(78.9%),并在尼日利亚(47.4%)和南非(26.3%)进行。研究最常评估巴氏涂片筛查(31.6%),并以曾接受过筛查(42.1%)或研究期间接受过筛查(36.8%)来衡量接受率。以教育为基础的干预措施最为常见(57.9%),最常针对 IBM 中进行筛查的知识/技能构建(68.4%)。在干预之前和之后,筛查的意愿都很高。干预后的筛查覆盖率范围为 1.7%至 99.2%,有 6 项研究(31.6%)报告了显著改善的筛查,覆盖率达到≥60%。
教育干预措施基本上没有效果,除了那些利用同伴或社区卫生教育者和移动健康实施策略的干预措施。两项经济激励干预措施是中等有效的,通过作用于参与者的工具性态度,但筛查覆盖率低于 20%。创新的服务提供方式,包括基于社区的自我采样,针对环境限制采取行动,努力使服务对妇女更具可及性和适宜性,是最有效的。本审查表明,进行筛查的意愿可能不是筛查行为的主要决定因素,这表明可能需要其他理论框架来更全面地了解撒哈拉以南非洲的宫颈癌筛查接受率,特别是对于卫生系统变革干预措施。