Department of Rheumatology, Leiden University Medical Center, Leiden, the Netherlands
Department of Rheumatology, Erasmus Medical Center, Rotterdam, the Netherlands.
RMD Open. 2020 May;6(1). doi: 10.1136/rmdopen-2020-001220.
Although current treatment guidelines for rheumatoid arthritis (RA) suggest tapering disease-modifying anti-rheumatic drugs (DMARDs), it is unclear whether DMARD-free remission (DFR) is an achievable and sustainable outcome. Therefore, we systematically reviewed the literature to determine the prevalence and sustainability of DFR and evaluated potential predictors for DFR.
A systematic literature search was performed in March 2019 in multiple databases. All clinical trials and observational studies reporting on discontinuation of DMARDs in RA patients in remission were included. Our quality assessment included a general assessment and assessment of the description of DFR. Prevalence of DFR and its sustainability and flares during tapering and after DMARD stop were summarised. Also, potential predictors for achieving DFR were reviewed.
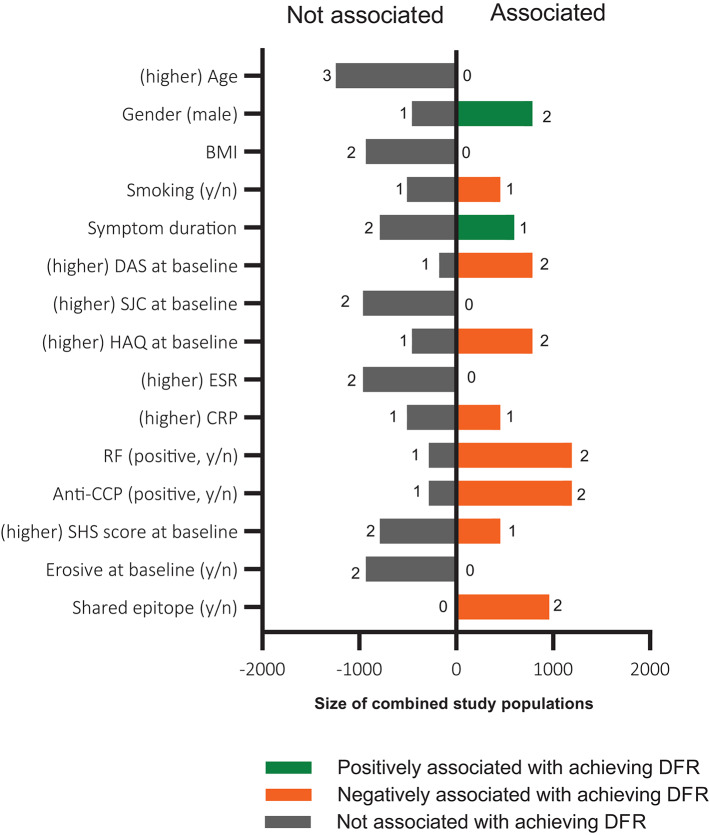
From 631 articles, 51 were included, comprising 14 clinical trials and 5 observational studies. DFR definition differed, especially for the duration of DMARD-free state. Considering only high- and moderate-quality studies, DFR was achieved in 5.0%-24.3% and sustained DFR (duration>12 months) in 11.6%-19.4% (both relative to the number of patients eligible for tapering). Flares occurred frequently during DMARD tapering (41.8%-75.0%) and in the first year after achieving DFR (10.4%-11.8%), while late flares, >1 year after DMARD-stop, were infrequent (0.3%-3.5%). Many patient characteristics lacked association with DFR. Absence of autoantibodies and shared epitope alleles increased the chance of achieving DFR.
DFR is achievable in RA and is sustainable in ~10%-20% of patients. DFR can become an important outcome measure for clinical trials and requires consistency in the definition. Considering the high rate of flares in the first year after DMARD stop, a DMARD-free follow-up of >12 months is advisable to evaluate sustainability.
尽管类风湿关节炎(RA)的现行治疗指南建议逐渐减少疾病修饰抗风湿药物(DMARD),但 DMARD 停药缓解(DFR)是否可实现和可持续仍不清楚。因此,我们系统地回顾了文献,以确定 DFR 的发生率和可持续性,并评估 DFR 的潜在预测因素。
2019 年 3 月在多个数据库中进行了系统文献检索。所有报告 RA 缓解患者停止 DMARD 的临床试验和观察性研究均被纳入。我们的质量评估包括对 DFR 的描述的一般评估和评估。总结了 DFR 的发生率及其可持续性以及在减少 DMARD 期间和停药后发生的flare。还回顾了实现 DFR 的潜在预测因素。
从 631 篇文章中,有 51 篇被纳入,包括 14 项临床试验和 5 项观察性研究。DFR 的定义不同,特别是 DMARD 无药状态的持续时间。仅考虑高质量和中等质量的研究,DFR 的实现率为 5.0%-24.3%,持续 DFR(持续时间>12 个月)的实现率为 11.6%-19.4%(均相对于有资格进行减量的患者人数)。在 DMARD 减量期间(41.8%-75.0%)和达到 DFR 后的第一年(10.4%-11.8%),flare 经常发生,而在 DMARD 停药>1 年后,晚期 flare (3.5%)很少见。许多患者特征与 DFR 缺乏关联。缺乏自身抗体和共享表位等位基因增加了实现 DFR 的机会。
RA 中可实现 DFR,在~10%-20%的患者中可持续。DFR 可以成为临床试验的重要结果指标,需要在定义上保持一致。考虑到 DMARD 停药后第一年 flare 的发生率较高,建议进行>12 个月的无 DMARD 随访,以评估可持续性。