Department of Nursing, Nishinomiya Kyoritsu Neurosurgical Hospital, 11-1 Imazuyamanaka-cho, Nishinomiya, Hyogo 663-8211, Japan.
Department of Palliative and Supportive Medicine, Aichi Medical University Hospital, 1-1 Yazakokarimata, Nagakute, Aichi 480-1195, Japan.
Nutrients. 2020 May 10;12(5):1365. doi: 10.3390/nu12051365.
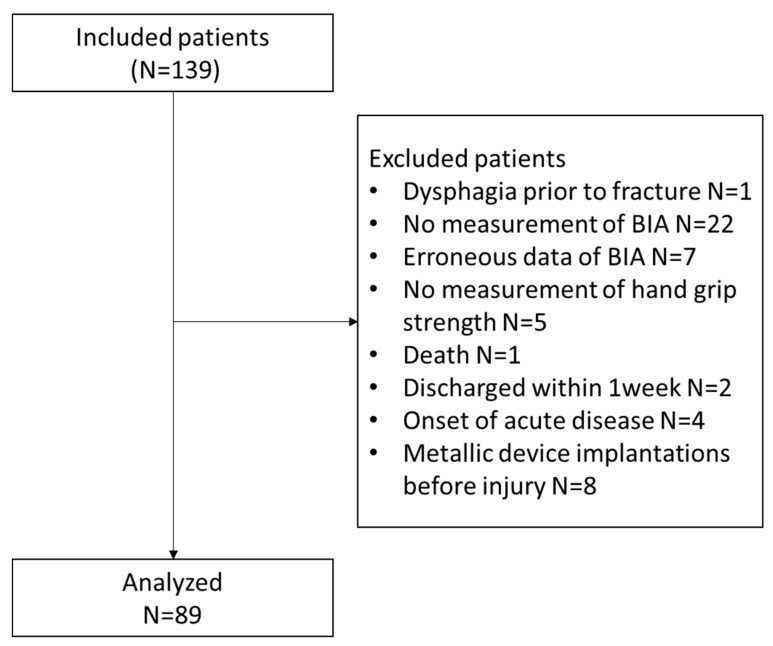
This study aimed to investigate the association between the development of dysphagia in patients with underlying sarcopenia and the prevalence of sarcopenic dysphagia in older patients following surgical treatment for hip fracture. Older female patients with hip fractures ( = 89) were studied. The data of skeletal muscle mass, hand-grip strength, and nutritional status were examined. The development of dysphagia postoperatively was graded using the Food Oral Intake Scale by a certified nurse in dysphagia nursing. The patients' mean age was 85.9 ± 6.5 years. The prevalence of sarcopenia was 76.4% at baseline. Of the 89 patients, 11 (12.3%) and 12 (13.5%) had dysphagia by day 7 of hospitalization and at discharge, respectively. All patients who developed dysphagia had underlying sarcopenia. Lower skeletal muscle mass index (SMI) (<4.7 kg/m) and grip strength (<8 kg) at baseline indicated a higher incidence of dysphagia on day 7 (p = 0.003 and Phi = 0.391) and at discharge (p = 0.001 and Phi = 0.448). Dysphagia developed after hip fracture surgery could be sarcopenic dysphagia, and worsening sarcopenia was a risk factor for dysphagia following hip fracture surgery. Clinicians and medical coworkers should become more aware of the risks of sarcopenic dysphagia. Early detection and preventive interventions for dysphagia should be emphasized.
本研究旨在探讨潜在的肌少症与老年髋部骨折患者术后吞咽困难的发展之间的关联,以及接受手术治疗的老年髋部骨折患者中肌少性吞咽困难的患病率。研究纳入了 89 例老年女性髋部骨折患者。检查了骨骼肌量、握力和营养状况的数据。术后吞咽困难的发展通过认证的吞咽障碍护理护士使用食物口腔摄入量表进行分级。患者的平均年龄为 85.9 ± 6.5 岁。基线时肌少症的患病率为 76.4%。在 89 例患者中,分别有 11 例(12.3%)和 12 例(13.5%)在住院第 7 天和出院时出现吞咽困难。所有发生吞咽困难的患者均存在潜在的肌少症。基线时骨骼肌量指数(SMI)较低(<4.7 kg/m)和握力较低(<8 kg)表明在第 7 天(p = 0.003 和 Phi = 0.391)和出院时(p = 0.001 和 Phi = 0.448)发生吞咽困难的发生率更高。髋部骨折手术后发生的吞咽困难可能是肌少性吞咽困难,且髋部骨折手术后吞咽困难的风险因素是肌少症恶化。临床医生和医疗同事应该更加意识到肌少性吞咽困难的风险。应强调对吞咽困难的早期检测和预防干预。