Adult Infectious Diseases Center, University Teaching Hospital, Lusaka, Zambia.
University of Alabama at Birmingham School of Medicine, Birmingham, AL, USA.
AIDS Res Ther. 2022 Feb 22;19(1):10. doi: 10.1186/s12981-022-00433-8.
Zambia recently achieved UNAIDS 90-90-90 treatment targets for HIV epidemic control; however, inpatient facilities continue to face a large burden of patients with advanced HIV disease and HIV-related mortality. Management of advanced HIV disease, following guidelines from outpatient settings, may be more difficult within complex inpatient settings. We evaluated adherence to HIV guidelines during hospitalization, including opportunistic infection (OI) screening, treatment, and prophylaxis.
We reviewed inpatient medical records of people living with HIV (PLHIV) admitted to the University Teaching Hospital in Lusaka, Zambia between December 1, 2018 and April 30, 2019. We collected data on patient demographics, antiretroviral therapy (ART), HIV biomarkers, and OI screening and treatment-including tuberculosis (TB), Cryptococcus, and OI prophylaxis with co-trimoxazole (CTX). Screening and treatment cascades were constructed based on the 2017 WHO Advanced HIV Guidelines.
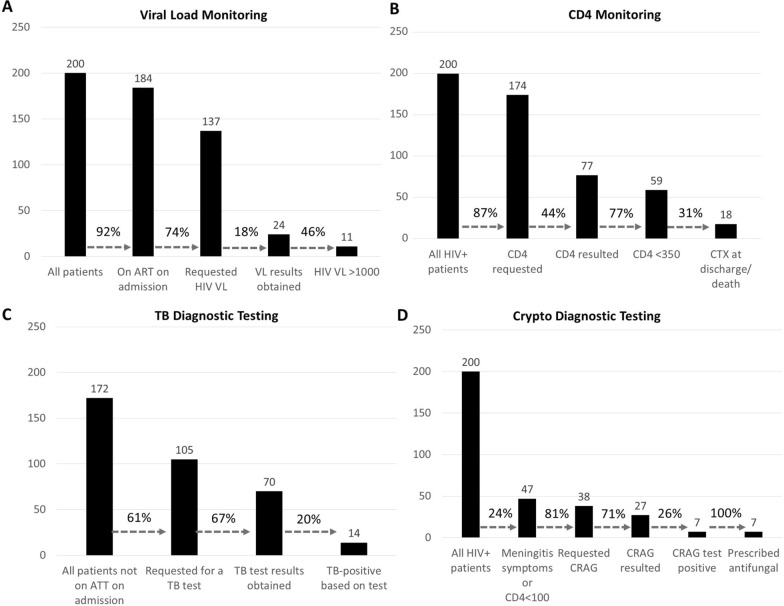
We reviewed files from 200 charts of patients with advanced HIV disease; of these 92% (184/200) had been on ART previously; 58.1% (107/184) for more than 12 months. HIV viral load (VL) testing was uncommon but half of VL results were high. 39% (77/200) of patients had a documented CD4 count result. Of the 172 patients not on anti-TB treatment (ATT) on admission, TB diagnostic tests (either sputum Xpert MTB/RIF MTB/RIF or urine TB-LAM) were requested for 105 (61%) and resulted for 60 of the 105 (57%). Nine of the 14 patients (64%) with a positive lab result for TB died before results were available. Testing for Cryptococcosis was performed predominantly in patients with symptoms of meningitis. Urine TB-LAM testing was rarely performed.
At a referral hospital in Zambia, CD4 testing was inconsistent due to laboratory challenges and this reduced recognition of AHD and implementation of AHD guidelines. HIV programs can potentially reduce mortality and identify PLHIV with retention and adherence issues through strengthening inpatient activities, including reflex VL testing, TB-LAM and serum CrAg during hospitalization.
赞比亚最近实现了联合国艾滋病规划署(UNAIDS)关于艾滋病毒流行控制的 90-90-90 治疗目标;然而,住院设施仍面临着大量晚期艾滋病毒疾病和与艾滋病毒相关的死亡患者的负担。在复杂的住院环境中,根据门诊环境的指南来管理晚期艾滋病毒疾病可能会更加困难。我们评估了住院期间对艾滋病毒指南的遵守情况,包括机会性感染(OI)筛查、治疗和预防。
我们回顾了 2018 年 12 月 1 日至 2019 年 4 月 30 日期间在赞比亚卢萨卡大学教学医院住院的艾滋病毒感染者(PLHIV)的住院病历。我们收集了患者人口统计学、抗逆转录病毒治疗(ART)、艾滋病毒生物标志物以及 OI 筛查和治疗的数据,包括结核病(TB)、隐球菌和复方磺胺甲噁唑(CTX)预防 OI。根据 2017 年世卫组织高级艾滋病毒指南构建了筛查和治疗级联。
我们审查了 200 份晚期艾滋病毒疾病患者病历,其中 92%(184/200)以前曾接受过 ART 治疗;58.1%(107/184)接受治疗时间超过 12 个月。HIV 病毒载量(VL)检测并不常见,但一半的 VL 结果都很高。39%(77/200)的患者有记录的 CD4 计数结果。在入院时未接受抗结核治疗(ATT)的 172 名患者中,有 105 名(61%)请求进行结核病诊断检测(Xpert MTB/RIF MTB/RIF 或尿液结核分枝杆菌潜伏感染快速检测(TB-LAM)),其中 60 名(57%)进行了检测。在有结核病实验室阳性结果的 14 名患者中,有 9 名(64%)在结果出来之前死亡。隐球菌病检测主要在有脑膜炎症状的患者中进行。尿液结核分枝杆菌潜伏感染快速检测很少进行。
在赞比亚的一家转诊医院,由于实验室挑战,CD4 检测不一致,这降低了对 AHD 的认识,并影响了 AHD 指南的实施。艾滋病毒规划可以通过加强住院活动,包括在住院期间进行反射性 VL 检测、TB-LAM 和血清 CrAg,来潜在地降低死亡率,并发现有保留和坚持问题的 PLHIV。