University of Virginia / Riverside, Radiosurgery Center, Newport News, VA, USA.
Department of Radiation Oncology, University of Virginia, Charlottesville, VA, USA.
Radiat Oncol. 2020 May 13;15(1):108. doi: 10.1186/s13014-020-01564-w.
This study evaluates the outcomes and toxicity of stereotactic body radiation therapy (SBRT) in ovarian cancer.
This retrospective analysis considered all patients treated with SBRT from 2009 to 2018 with a primary ovarian tumor. Follow-up included PET-CT and CT scans at 2-3 month intervals. Statistical analysis primarily consisted of univariate analysis, Cox proportional hazards analysis, and the Kaplan-Meier method.
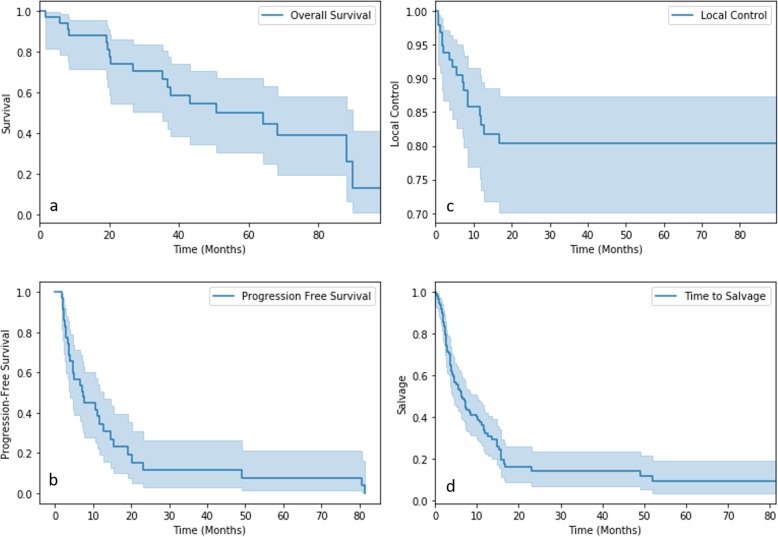
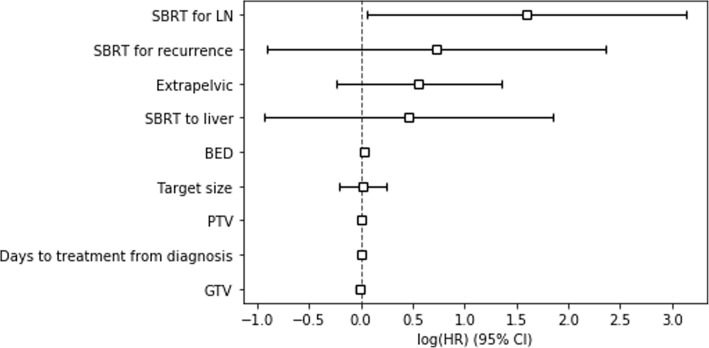
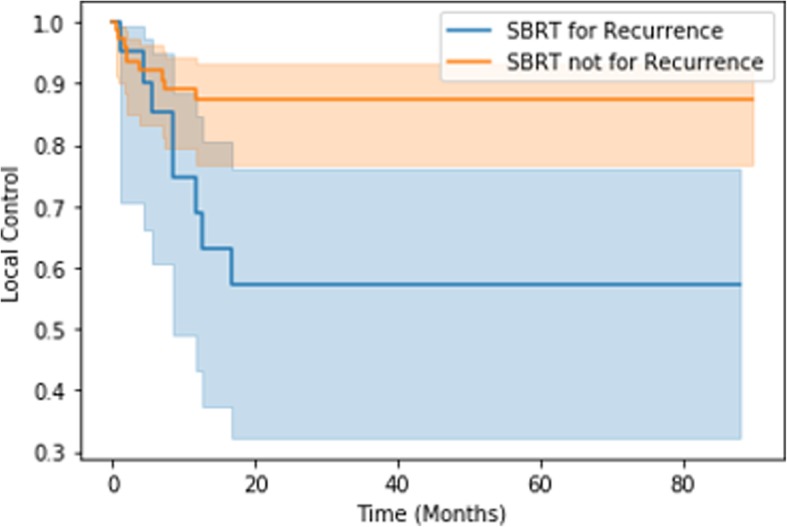
The study included 35 patients with 98 treatments for lymph nodes (51), local recurrence (21), and de novo solid metastases (26). Median biologically effective dose (BED), gross tumor volume, and planning target volume were 38.40 Gy, 10.41 cc, and 25.21 cc, respectively. 52 lesions showed complete radiographic response, and two-year local control was 80%. Median overall survival (OS) was 35.2 months, and two-year progression-free survival (PFS) was 12%. On univariate analysis, Eastern Cooperative Oncology Group performance status > 0 was predictive of decreased OS (p = 0.0024) and PFS (p = 0.044). Factors predictive of local failure included lower BED (p = 0.016), treatment for recurrence (p = 0.029), and higher pre-treatment SUV (p = 0.026). Kaplan-Meier analysis showed BED ≤35 Gy (p < 0.005) and treatment for recurrence (p = 0.01) to be predictive of local failure. On Cox proportional hazards analysis, treatment of lymph nodes was predictive of complete radiographic response (hazard ratio (HR) = 4.95), as was higher BED (HR = 1.03). Toxicity included 27 cases of grade < 3 toxicity, and one grade 5 late toxicity of GI bleed from a radiation therapy-induced duodenal ulcer.
SBRT provides durable local control with minimal toxicity in ovarian cancer, especially with BED > 35 Gy and treatment for lymph nodes.
本研究评估了立体定向体放射治疗(SBRT)在卵巢癌中的疗效和毒性。
本回顾性分析纳入了 2009 年至 2018 年间接受 SBRT 治疗的原发性卵巢肿瘤患者。随访包括 PET-CT 和 CT 扫描,间隔 2-3 个月进行一次。统计分析主要包括单因素分析、Cox 比例风险分析和 Kaplan-Meier 法。
本研究纳入了 35 例患者,98 次治疗用于治疗淋巴结(51 次)、局部复发(21 次)和新发实体转移(26 次)。中位生物有效剂量(BED)、大体肿瘤体积和计划靶区体积分别为 38.40Gy、10.41cc 和 25.21cc。52 处病灶完全显示放射性反应,两年局部控制率为 80%。中位总生存期(OS)为 35.2 个月,两年无进展生存期(PFS)为 12%。单因素分析显示,东部肿瘤协作组体能状态(ECOG PS)>0 与 OS(p=0.0024)和 PFS(p=0.044)降低相关。局部失败的预测因素包括较低的 BED(p=0.016)、治疗复发(p=0.029)和较高的治疗前 SUV(p=0.026)。Kaplan-Meier 分析显示,BED≤35Gy(p<0.005)和治疗复发(p=0.01)与局部失败相关。Cox 比例风险分析显示,治疗淋巴结与完全放射性反应相关(风险比(HR)=4.95),BED 较高(HR=1.03)也是如此。毒性包括 27 例<3 级毒性,1 例 5 级迟发性毒性为放射性治疗引起的十二指肠溃疡出血。
SBRT 在卵巢癌中提供了持久的局部控制,且毒性最小,特别是 BED>35Gy 和治疗淋巴结。