School of Pharmacy, Faculty of Medicine, The Chinese University of Hong Kong, Shatin, NT, China (Hong Kong).
JMIR Mhealth Uhealth. 2020 Jul 6;8(7):e17846. doi: 10.2196/17846.
Telemonitoring-guided interventional management reduces the need for hospitalization and mortality of patients with chronic heart failure (CHF).
This study aimed to analyze the cost-effectiveness of usual care with and without telemonitoring-guided management in patients with CHF discharged from the hospital, from the perspective of US health care providers.
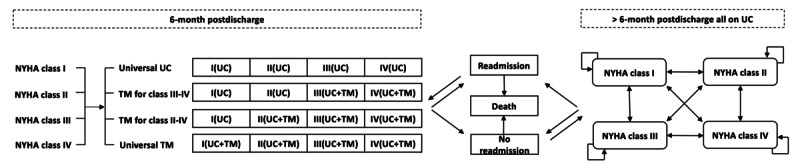
A lifelong Markov model was designed to estimate outcomes of (1) usual care alone for all postdischarge patients with CHF (New York Heart Association [NYHA] class I-IV), (2) usual care and telemonitoring for all postdischarge patients with CHF, (3) usual care for all postdischarge patients with CHF and telemonitoring for patients with NYHA class III to IV, and (4) usual care for all postdischarge patients with CHF plus telemonitoring for patients with NYHA class II to IV. Model inputs were derived from the literature and public data. Sensitivity analyses were conducted to assess the robustness of model. The primary outcomes were total direct medical cost, quality-adjusted life years (QALYs), and incremental cost-effectiveness ratio (ICER).
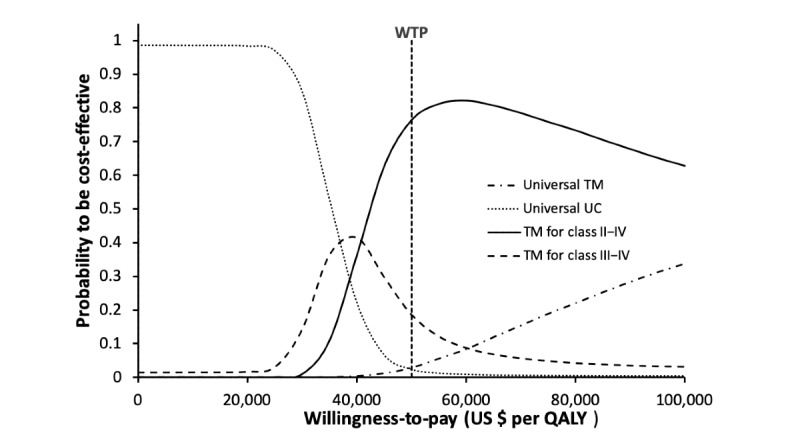
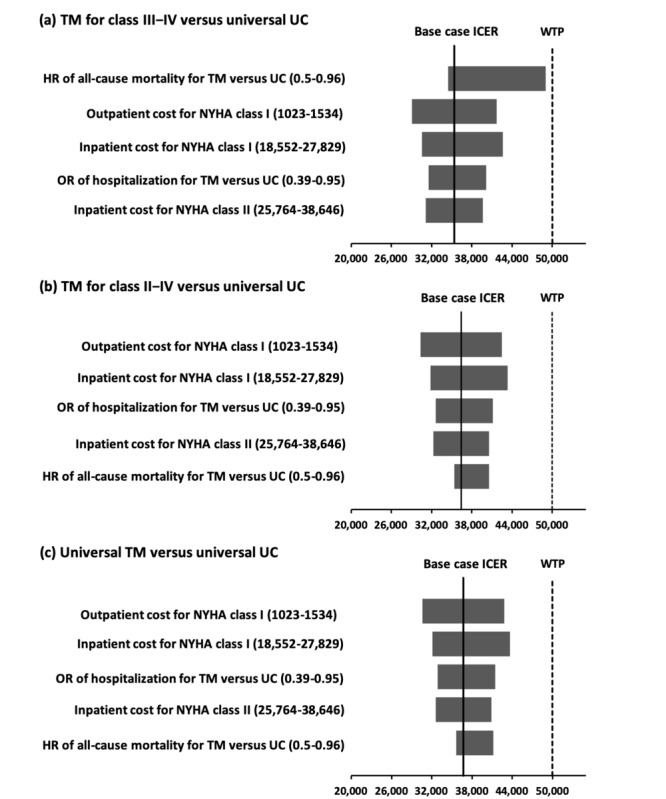
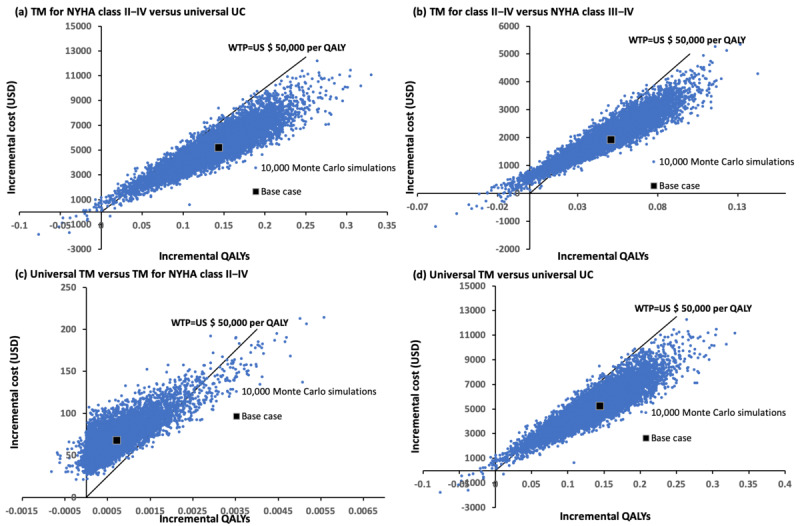
In the base case analysis, universal telemonitoring group gained the highest QALYs (6.2967 QALYs), followed by the telemonitoring for NYHA class II to IV group (6.2960 QALYs), the telemonitoring for NYHA class III to IV group (6.2450 QALYs), and the universal usual care group (6.1530 QALYs). ICERs of the telemonitoring for NYHA class III to IV group (US $35,393 per QALY) and the telemonitoring for NYHA class II to IV group (US $38,261 per QALY) were lower than the ICER of the universal telemonitoring group (US $100,458 per QALY). One-way sensitivity analysis identified five critical parameters: odds ratio of hospitalization for telemonitoring versus usual care, hazard ratio of all-cause mortality for telemonitoring versus usual care, CHF hospitalization cost and monthly outpatient costs for NYHA class I, and CHF hospitalization cost for NYHA class II. In probabilistic sensitivity analysis, probabilities of the universal telemonitoring, telemonitoring for NYHA class II to IV, telemonitoring for NYHA class III to IV, and universal usual care groups to be accepted as cost-effective at US $50,000 per QALY were 2.76%, 76.31%, 18.6%, and 2.33%, respectively.
Usual care for all discharged patients with CHF plus telemonitoring-guided management for NYHA class II to IV patients appears to be the preferred cost-effective strategy.
远程监测指导下的介入管理可降低慢性心力衰竭(CHF)患者的住院需求和死亡率。
本研究旨在从美国医疗保健提供者的角度分析出院后 CHF 患者接受常规护理加与不加远程监测指导管理的成本效益。
设计了一个终生 Markov 模型,以评估以下四种方案的结果:(1)所有 NYHA 分级 I-IV 级的出院后 CHF 患者仅接受常规护理;(2)所有出院后 CHF 患者均接受常规护理和远程监测指导管理;(3)所有出院后 CHF 患者仅接受常规护理,NYHA 分级 III-IV 级患者接受远程监测指导管理;(4)所有出院后 CHF 患者均接受常规护理加远程监测指导管理,NYHA 分级 II-IV 级患者接受远程监测指导管理。模型输入源自文献和公共数据。进行敏感性分析以评估模型的稳健性。主要结局指标是总直接医疗成本、质量调整生命年(QALY)和增量成本效益比(ICER)。
在基础案例分析中,普遍远程监测组获得了最高的 QALY(6.2967 QALY),其次是 NYHA 分级 II-IV 组(6.2960 QALY)、NYHA 分级 III-IV 组(6.2450 QALY)和普遍常规护理组(6.1530 QALY)。NYHA 分级 III-IV 组(每 QALY 35393 美元)和 NYHA 分级 II-IV 组(每 QALY 38261 美元)的远程监测 ICER 低于普遍远程监测组(每 QALY 100458 美元)。单向敏感性分析确定了五个关键参数:与常规护理相比,远程监测的住院率比值、与常规护理相比,远程监测的全因死亡率比值、NYHA 分级 I 的 CHF 住院费用和每月门诊费用、NYHA 分级 II 的 CHF 住院费用。在概率敏感性分析中,普遍远程监测、NYHA 分级 II-IV 远程监测、NYHA 分级 III-IV 远程监测和普遍常规护理组在 50000 美元/QALY 时被接受为具有成本效益的概率分别为 2.76%、76.31%、18.6%和 2.33%。
对于所有出院的 CHF 患者,给予常规护理加 NYHA 分级 II-IV 患者的远程监测指导管理似乎是一种具有成本效益的首选策略。