Department of General Internal Medicine, Inselspital, Bern University Hospital, University of Bern, Bern, Switzerland.
CTU Bern, University of Bern, Bern, Switzerland.
PLoS One. 2020 May 14;15(5):e0233082. doi: 10.1371/journal.pone.0233082. eCollection 2020.
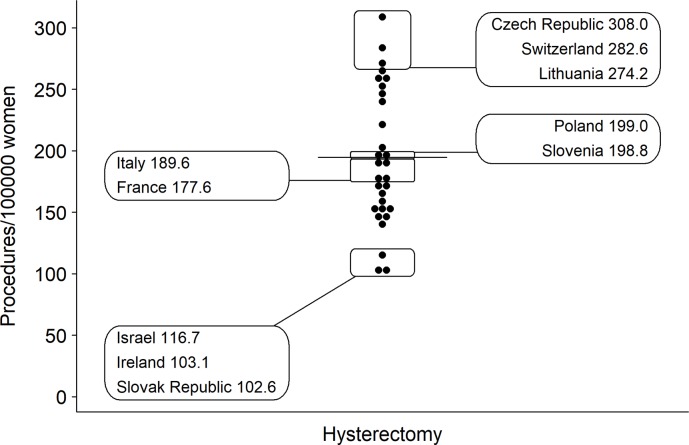
Hysterectomy is the last treatment option for benign uterine diseases, and vaginal hysterectomy is preferred over more invasive techniques. We assessed the regional variation in hysterectomy rates for benign uterine diseases across Switzerland and explored potential determinants of variation.
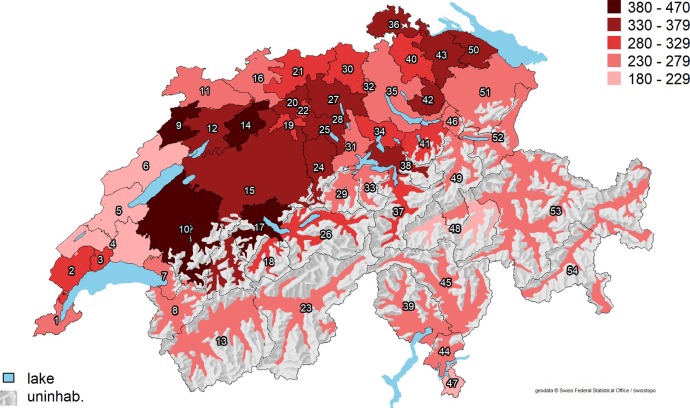
We conducted a population-based analysis using patient discharge data from all Swiss hospitals between 2013 and 2016. Hospital service areas (HSAs) for hysterectomies were derived by analyzing patient flows. We calculated age-standardized mean procedure rates and measures of regional variation (extremal quotient [EQ], highest divided by lowest rate) and systematic component of variation [SCV]). We estimated the reduction in the variance of crude hysterectomy rates across HSAs in multilevel regression models, with incremental adjustment for procedure year, age, cultural/socioeconomic factors, burden of disease, and density of gynecologists.
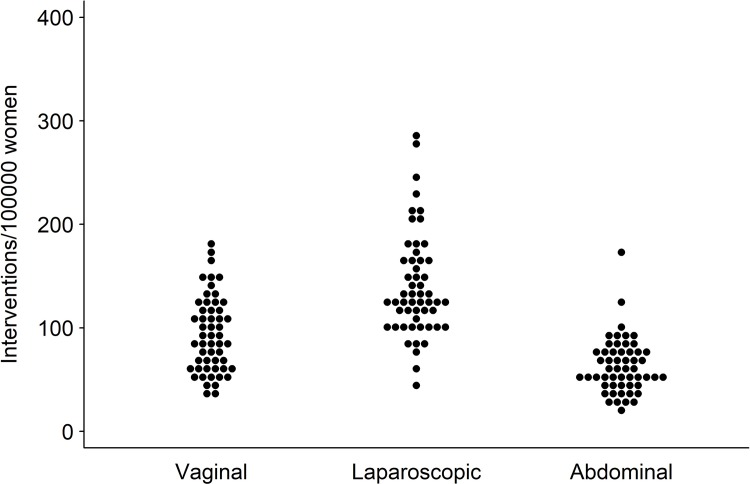
Overall, 40,211 hysterectomies from 54 HSAs were analyzed. The mean age-standardized hysterectomy rate was 298/100,000 women (range 186-456). While the variation in overall procedure rate was moderate (EQ 2.5, SCV 3.7), we found a very high procedure-specific variation (EQ vaginal 5.0, laparoscopic 6.3, abdominal 8.0; SCV vaginal 17.5, laparoscopic 11.2, abdominal 16.9). Adjusted for procedure year, demographic, cultural, and sociodemographic factors, a large share (64%) of the variance remained unexplained (vaginal 63%, laparoscopic 85%, abdominal 70%). The main determinants of variation were socioeconomic/cultural factors. Burden of disease and the density of gynecologists was not associated with procedure rates.
Switzerland has a very high regional variation in vaginal, laparoscopic, and abdominal hysterectomy for benign uterine disease. After adjustment for potential determinants of variation including demographic factors, socioeconomic and cultural factors, burden of disease, and the density of gynecologists, two thirds of the variation remain unexplained.
子宫切除术是治疗良性子宫疾病的最后一种治疗选择,并且阴道子宫切除术优于更具侵入性的技术。我们评估了瑞士各地良性子宫疾病子宫切除术率的区域差异,并探讨了变化的潜在决定因素。
我们使用 2013 年至 2016 年期间所有瑞士医院的患者出院数据进行了基于人群的分析。通过分析患者流量得出了用于子宫切除术的医院服务区 (HSA)。我们计算了年龄标准化的平均手术率和区域差异的衡量标准(极值比 [EQ],最高与最低比率)和系统变异成分 [SCV])。我们使用多水平回归模型估计了在 HSA 之间,通过逐步调整手术年份、年龄、文化/社会经济因素、疾病负担和妇科医生密度,对原始子宫切除术率方差的减少。
总体而言,分析了来自 54 个 HSA 的 40,211 例子宫切除术。年龄标准化的子宫切除术率平均为 298/100,000 名女性(范围 186-456)。虽然整体手术率的变化适中(EQ 2.5,SCV 3.7),但我们发现手术特异性变化非常高(EQ 阴道 5.0,腹腔镜 6.3,腹部 8.0;SCV 阴道 17.5,腹腔镜 11.2,腹部 16.9)。调整手术年份、人口统计学、文化和社会人口统计学因素后,仍有很大一部分(64%)方差未得到解释(阴道 63%,腹腔镜 85%,腹部 70%)。变化的主要决定因素是社会经济/文化因素。疾病负担和妇科医生的密度与手术率无关。
瑞士良性子宫疾病的阴道、腹腔镜和腹部子宫切除术的区域差异非常大。调整变化的潜在决定因素(包括人口统计学因素、社会经济和文化因素、疾病负担以及妇科医生的密度)后,仍有三分之二的差异无法解释。