Yasumura Kaori, Abe Haruhiko, Iida Yoshinori, Kato Taishi, Nakamura Masayuki, Toriyama Chieko, Nishida Hiroki, Idemoto Akiko, Shinouchi Kazuya, Mishima Tsuyoshi, Awata Masaki, Date Motoo, Ueda Yasunori, Uematsu Masaaki, Koretsune Yukihiro
Cardiovascular Division, National Hospital Organization Osaka National Hospital, Osaka, Japan.
ESC Heart Fail. 2020 Aug;7(4):1801-1808. doi: 10.1002/ehf2.12743. Epub 2020 May 14.
Nutritional status as well as physical capacity is related to prognosis in patients with heart failure. The purpose of this study was to explore a simple prognostic indicator in patients with acute decompensated heart failure (ADHF) by including both nutritional status and physical capacity.
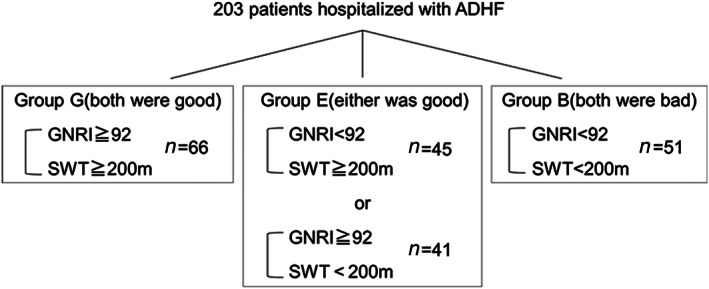
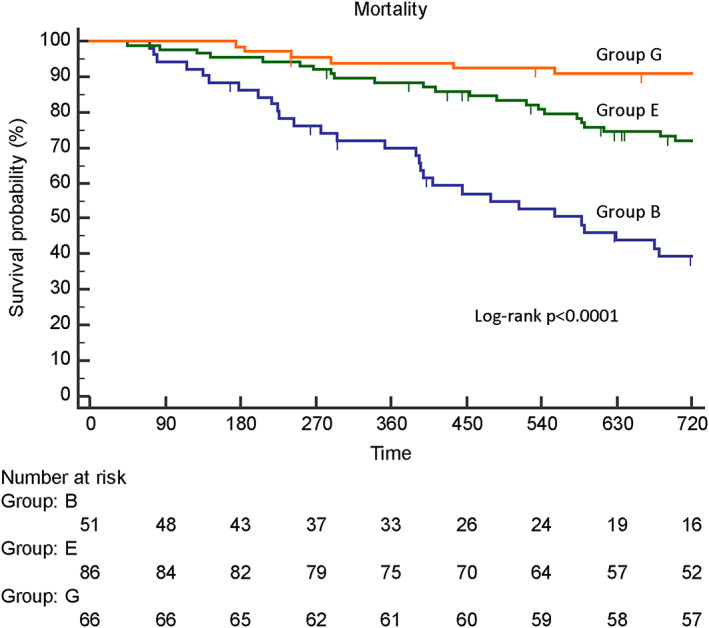
Patients hospitalized with ADHF (N = 203; mean age, 81 years) were enrolled. We evaluated the geriatric nutritional risk index (GNRI) on hospital admission and at discharge. A GNRI score < 92 was defined as malnutrition. Physical capacity was evaluated by simple walking test to determine if patients could walk 200 m, with a Borg scale score ≤ 13, without critical changes in vital signs. Primary endpoints were mortality and heart failure rehospitalization within 2 years. A total of 49% and 48% of patients showed malnutrition on admission and at discharge, respectively. Malnutrition at discharge was more strongly related to mortality [hazard ratio (HR) 3.382, 95% confidence interval (CI) 1.900-6.020, P < 0.0001)] than that on admission (HR 2.448, 95% CI 1.442-4.157, P = 0.001) by univariable analysis. Malnutrition at discharge was related to mortality (HR 2.370, 95% CI 1.166-4.814, P = 0.02), but malnutrition on admission was not related (HR 1.538, 95% CI 0.823-2.875, P = 0.18) by multivariable analysis. Almost half of patients (45%) could not walk 200 m, which was significantly related to mortality by univariable analysis (HR 3.303, 95% CI 1.905-5.727, P < 0.0001), but was not by multivariable analysis (HR 1.990, 95% CI 0.999-3.962, P = 0.05). The combined index including both GNRI and simple walking test was an independent and stronger predictor of mortality than either index alone by multivariable analysis (HR 2.249, 95% CI 1.362-3.716, P < 0.01). Neither malnutrition nor low physical capacity was related to heart failure rehospitalization by univariable analysis (HR 0.702, 95% CI 0.483-1.020, P = 0.06; HR 1.047, 95% CI 0.724-1.515, P = 0.81, respectively). Malnutrition at discharge significantly reduced heart failure rehospitalization by multivariable analysis (HR 0.431, 95% CI 0.266-0.698, P < 0.01). When patients were classified into Group G (both nutritional status and physical capacity at discharge were good), Group E (either was good), and Group B (both were bad), mortality rates were significantly different among the groups (log rank P < 0.0001).
A simple indicator including both nutritional status and physical capacity may predict 2 year mortality in elderly patients with ADHF.
营养状况以及身体机能与心力衰竭患者的预后相关。本研究的目的是通过纳入营养状况和身体机能来探索急性失代偿性心力衰竭(ADHF)患者的一个简单预后指标。
纳入因ADHF住院的患者(N = 203;平均年龄81岁)。我们在入院时和出院时评估老年营养风险指数(GNRI)。GNRI评分<92被定义为营养不良。通过简单步行试验评估身体机能,以确定患者是否能在生命体征无严重变化的情况下步行200米,Borg量表评分≤13。主要终点是2年内的死亡率和心力衰竭再住院率。分别有49%和48%的患者在入院时和出院时存在营养不良。单变量分析显示,出院时的营养不良比入院时的营养不良与死亡率的相关性更强[风险比(HR)3.382,95%置信区间(CI)1.900 - 6.020,P < 0.0001](HR 2.448,95% CI 1.442 - 4.157,P = 0.001)。多变量分析显示,出院时的营养不良与死亡率相关(HR 2.370,95% CI 1.166 - 4.814,P = 0.02),但入院时的营养不良与死亡率无关(HR 1.538,95% CI 0.823 - 2.875,P = 0.18)。几乎一半的患者(45%)无法步行200米,单变量分析显示这与死亡率显著相关(HR 3.303,95% CI 1.905 - 5.727,P < 0.0001),但多变量分析显示无关(HR 1.990,95% CI 0.999 - 3.962,P = 0.05)。多变量分析显示,包括GNRI和简单步行试验的综合指标比单独的任何一个指标都是更独立且更强的死亡率预测指标(HR 2.249,95% CI 1.362 - 3.716,P < 0.01)。单变量分析显示,营养不良和身体机能低下均与心力衰竭再住院率无关(HR 0.702,95% CI 0.483 - 1.020,P = 0.06;HR 1.047,95% CI 0.724 - 1.515,P = 0.81)。多变量分析显示,出院时的营养不良显著降低了心力衰竭再住院率(HR 0.431,95% CI 0.266 - 0.698,P < 0.01)。当患者被分为G组(出院时营养状况和身体机能均良好)、E组(其中一项良好)和B组(两者均差)时,各组的死亡率存在显著差异(对数秩检验P < 0.0001)。
一个包括营养状况和身体机能的简单指标可能预测老年ADHF患者的2年死亡率。