Department of Radiology, Haeundae Paik Hospital, Inje University College of Medicine, Busan, Korea.
Department of Radiology, Seoul Metropolitan Government-Seoul National University Boramae Medical Center, Seoul, Korea.
Korean J Radiol. 2020 Jun;21(6):707-716. doi: 10.3348/kjr.2019.0629.
To evaluate pharmacokinetic variables from contrast-enhancing lesions (CELs) and non-enhancing T2 high signal intensity lesions (NE-T2HSILs) on dynamic contrast-enhanced (DCE) magnetic resonance (MR) imaging for predicting progression-free survival (PFS) in glioblastoma (GBM) patients.
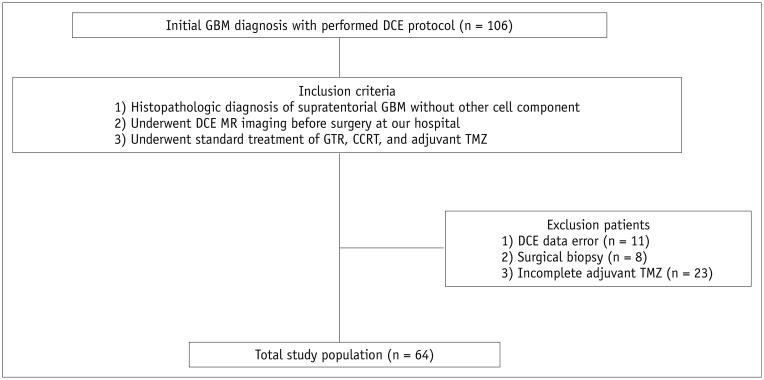
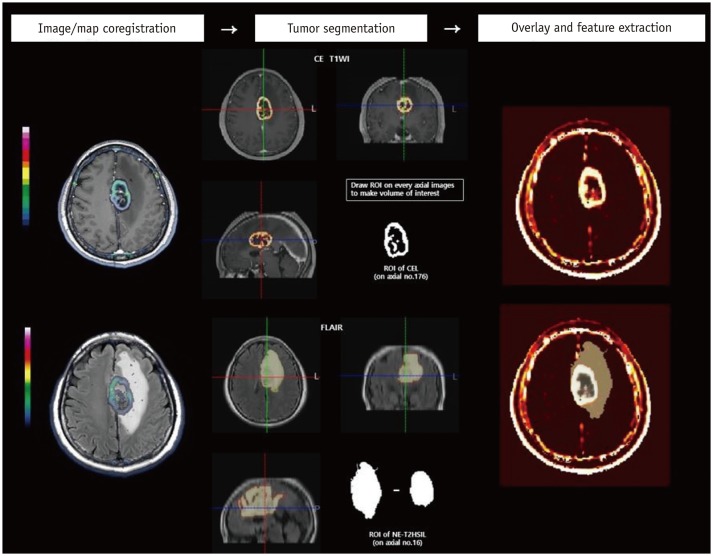
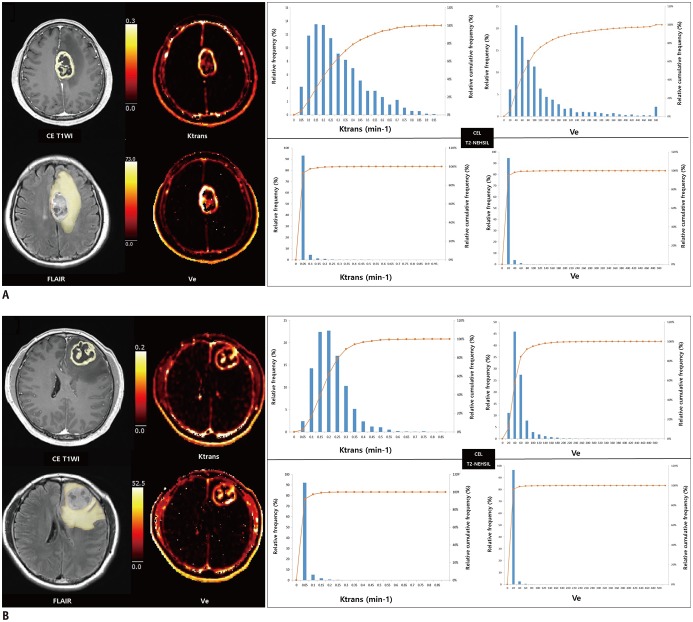
Sixty-four GBM patients who had undergone preoperative DCE MR imaging and received standard treatment were retrospectively included. We analyzed the pharmacokinetic variables of the volume transfer constant (Ktrans) and volume fraction of extravascular extracellular space within the CEL and NE-T2HSIL of the entire tumor. Univariate and multivariate Cox regression analyses were performed using preoperative clinical characteristics, pharmacokinetic variables of DCE MR imaging, and postoperative molecular biomarkers to predict PFS.
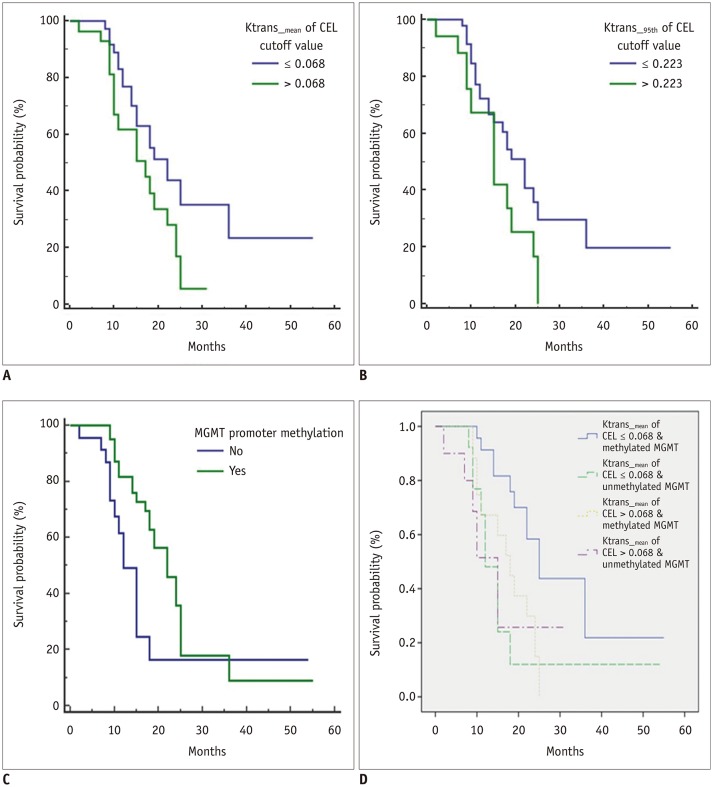
The increased mean Ktrans of the CEL, increased 95th percentile Ktrans of the CELs, and absence of methylated O⁶-methylguanine-DNA methyltransferase promoter were relevant adverse variables for PFS in the univariate analysis ( = 0.041, = 0.032, and = 0.083, respectively). The Kaplan-Meier survival curves demonstrated that PFS was significantly shorter in patients with a mean Ktrans of the CEL > 0.068 and 95th percentile Ktrans of the CEL>0.223 (log-rank = 0.038 and = 0.041, respectively). However, only mean Ktrans of the CEL was significantly associated with PFS ( = 0.024; hazard ratio, 553.08; 95% confidence interval, 2.27-134756.74) in the multivariate Cox proportional hazard analysis. None of the pharmacokinetic variables from NE-T2HSILs were significantly related to PFS.
Among the pharmacokinetic variables extracted from CELs and NE-T2HSILs on preoperative DCE MR imaging, the mean Ktrans of CELs exhibits potential as a useful imaging predictor of PFS in GBM patients.
评估对比增强病变(CEL)和非增强 T2 高信号强度病变(NE-T2HSIL)的动态对比增强(DCE)磁共振成像(MR)中的药代动力学变量,以预测胶质母细胞瘤(GBM)患者的无进展生存期(PFS)。
回顾性纳入 64 例接受术前 DCE-MR 成像且接受标准治疗的 GBM 患者。我们分析了整个肿瘤的 CEL 和 NE-T2HSIL 的容积转移常数(Ktrans)和血管外细胞外间隙体积分数的药代动力学变量。使用术前临床特征、DCE-MR 成像的药代动力学变量和术后分子生物标志物进行单变量和多变量 Cox 回归分析,以预测 PFS。
CEL 的平均 Ktrans 增加、CEL 的 95%百分位数 Ktrans 增加以及甲基化 O⁶-甲基鸟嘌呤-DNA 甲基转移酶启动子缺失是 PFS 的不良单变量因素( = 0.041、 = 0.032 和 = 0.083)。Kaplan-Meier 生存曲线表明,CEL 平均 Ktrans>0.068 和 CEL 95%百分位数 Ktrans>0.223 的患者 PFS 显著缩短(对数秩检验=0.038 和 =0.041)。然而,只有 CEL 的平均 Ktrans 与 PFS 显著相关( = 0.024;危险比,553.08;95%置信区间,2.27-134756.74)。在多变量 Cox 比例风险分析中,来自 NE-T2HSIL 的药代动力学变量均与 PFS 无显著相关性。
在术前 DCE-MR 成像中从 CEL 和 NE-T2HSIL 提取的药代动力学变量中,CEL 的平均 Ktrans 作为预测 GBM 患者 PFS 的一种有价值的影像学预测因子具有潜力。