Medecins Sans Frontieres OCBA, Barcelona, Spain.
Centre for Global Health Research, Usher Institute, University of Edinburgh, Edinburgh, UK.
BMC Pregnancy Childbirth. 2020 May 14;20(1):298. doi: 10.1186/s12884-020-02995-9.
To evaluate the perinatal status of neonates delivered by assisted vaginal delivery (AVD) versus second-stage caesarean birth (CS).
A 5-year retrospective study was conducted in a tertiary hospital. Data was analyzed with IBM SPSS® version 25.0 statistical software using descriptive/inferential statistics.
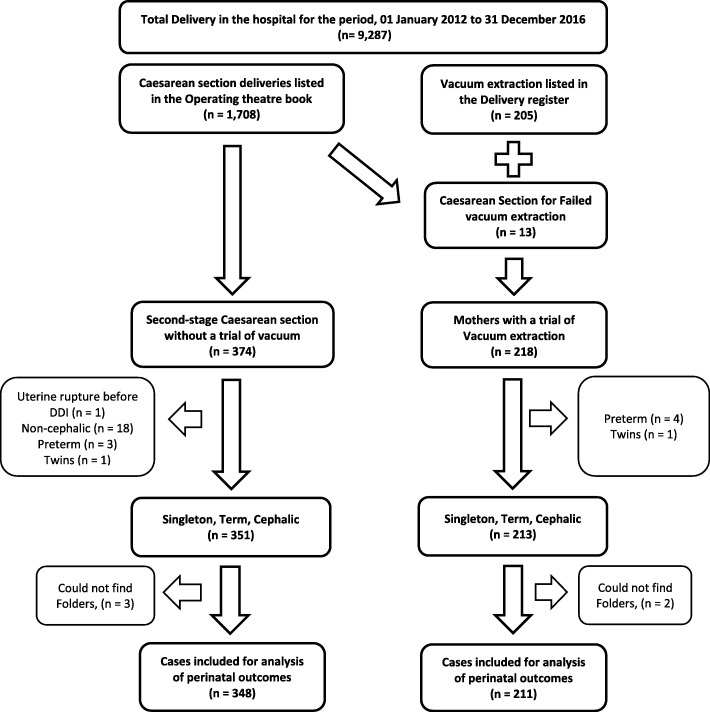
A total of 559 births met the inclusion criteria; AVD (211; 37.7%) and second-stage CS (348; 62.3%). Over 80% of the women were aged 20-34 years: 185 (87.7%) for the AVD group, and 301 (86.5%) for the second-stage CS group. More than half of the women were parous: 106 (50.2%) for the AVD group, and 184 (52.9%) for the second-stage CS group. The commonest indication for intervention in both groups is delayed second stage: 178 (84.4%) in the AVD group, and 239 (68.9%) in the second-stage CS group. There was a statistically significant difference in decision to delivery interval (DDI) between both groups: 197 (93.4%) women in the AVD group had DDI of less than 30 min and 21 women (6.0%) in the CS group had a DDI of less than 30 min (p < 0.001). During the DDI, there were 3 (1.4%) intra-uterine foetal deaths (IUFD) in the AVD and 19 (5.5%) in the CS group (p = 0.023). After adjusting for co-variates, there were statistically significant differences between the AVD and CS groups in the foetal death during DDI (p = 0.029) and perinatal deaths (p = 0.040); but no statistically significant differences in severe perinatal outcomes (p = 0.811), APGAR scores at 5th minutes (p = 0.355), and admission into the NICU (p = 0.946). After adjusting for co-variates, use of AVD was significantly associated with the level of experience of the care provider, with resident (junior) doctors less likely to opt for AVD than CS (aOR = 0.45, 95% CI: 0.29-0.70).
Second-stage CS when compared with AVD was not associated with improved perinatal outcomes. AVD is a practical option for reducing the rising Caesarean delivery rates without compromising the clinical status of the newborn.
评估经阴道辅助分娩(AVD)与第二产程剖宫产(CS)新生儿的围生期状况。
在一家三级医院进行了一项为期 5 年的回顾性研究。使用 IBM SPSS® 版本 25.0 统计软件对数据进行分析,采用描述性/推断性统计。
共有 559 例分娩符合纳入标准;AVD(211;37.7%)和第二产程 CS(348;62.3%)。超过 80%的女性年龄在 20-34 岁之间:AVD 组 185 例(87.7%),第二产程 CS 组 301 例(86.5%)。超过一半的女性是经产妇:AVD 组 106 例(50.2%),第二产程 CS 组 184 例(52.9%)。两组最常见的干预指征是第二产程延长:AVD 组 178 例(84.4%),第二产程 CS 组 239 例(68.9%)。两组的分娩决策间隔(DDI)有统计学显著差异:AVD 组 197 例(93.4%)DDI 小于 30 分钟,CS 组 21 例(6.0%)DDI 小于 30 分钟(p<0.001)。在 DDI 期间,AVD 组有 3 例(1.4%)胎儿宫内死亡(IUFD),CS 组有 19 例(5.5%)(p=0.023)。调整协变量后,AVD 组和 CS 组在 DDI 期间胎儿死亡(p=0.029)和围产儿死亡(p=0.040)方面有统计学显著差异;但严重围产儿结局(p=0.811)、第 5 分钟时的 APGAR 评分(p=0.355)和入住新生儿重症监护病房(p=0.946)无统计学显著差异。调整协变量后,使用 AVD 与护理提供者的经验水平显著相关,与 CS 相比,住院医师(初级)医生不太可能选择 AVD(aOR=0.45,95%CI:0.29-0.70)。
与 AVD 相比,第二产程 CS 并未改善围生期结局。AVD 是降低剖宫产率而不影响新生儿临床状况的实用选择。