Comparative and Experimental Medicine College of Veterinary Medicine The University of Tennessee Knoxville TN.
Department of Geography The University of Tennessee Knoxville TN.
J Am Heart Assoc. 2020 Jun 2;9(11):e012712. doi: 10.1161/JAHA.119.012712. Epub 2020 May 19.
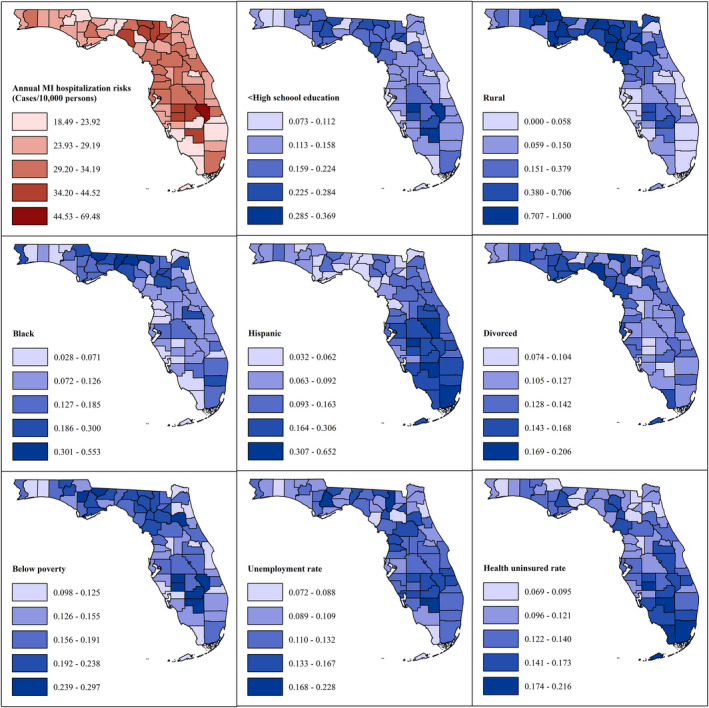
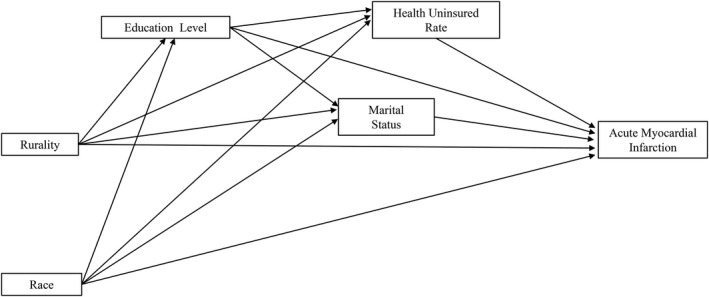
Background Identifying social determinants of myocardial infarction (MI) hospitalizations is crucial for reducing/eliminating health disparities. Therefore, our objectives were to identify sociodemographic determinants of MI hospitalization risks and to assess if the impacts of these determinants vary by geographic location in Florida. Methods and Results This is a retrospective ecologic study at the county level. We obtained data for principal and secondary MI hospitalizations for Florida residents for the 2005-2014 period and calculated age- and sex-adjusted MI hospitalization risks. We used a multivariable negative binomial model to identify sociodemographic determinants of MI hospitalization risks and a geographically weighted negative binomial model to assess if the strength of associations vary by location. There were 645 935 MI hospitalizations (median age, 72 years; 58.1%, men; 73.9%, white). Age- and sex-adjusted risks ranged from 18.49 to 69.48 cases/10 000 persons, and they were significantly higher in counties with low education levels (risk ratio [RR]=1.033, <0.0001) and high divorce rate (RR, 0.995; =0.018). However, they were significantly lower in counties with high proportions of rural (RR, 0.996; <0.0001), black (RR, 1.026; =0.032), and uninsured populations (RR, 0.983; =0.040). Associations of MI hospitalization risks with education level and uninsured rate varied geographically ( for non-stationarity test=0.001 and 0.043, respectively), with strongest associations in southern Florida (RR for <high school education, 1.036-1.041; RR for uninsured rate, 0.971-0.976). Conclusions Black race, divorce, rural residence, low education level, and lack of health insurance were significant determinants of MI hospitalization risks, but associations with the latter 2 were stronger in southern Florida. Thus, interventions for addressing MI hospitalization risks need to prioritize these populations and allocate resources based on empirical evidence from global and local models for maximum efficiency and effectiveness.
确定心肌梗死 (MI) 住院的社会决定因素对于减少/消除健康差距至关重要。因此,我们的目标是确定 MI 住院风险的社会人口决定因素,并评估这些决定因素在佛罗里达州的地理位置是否存在差异。
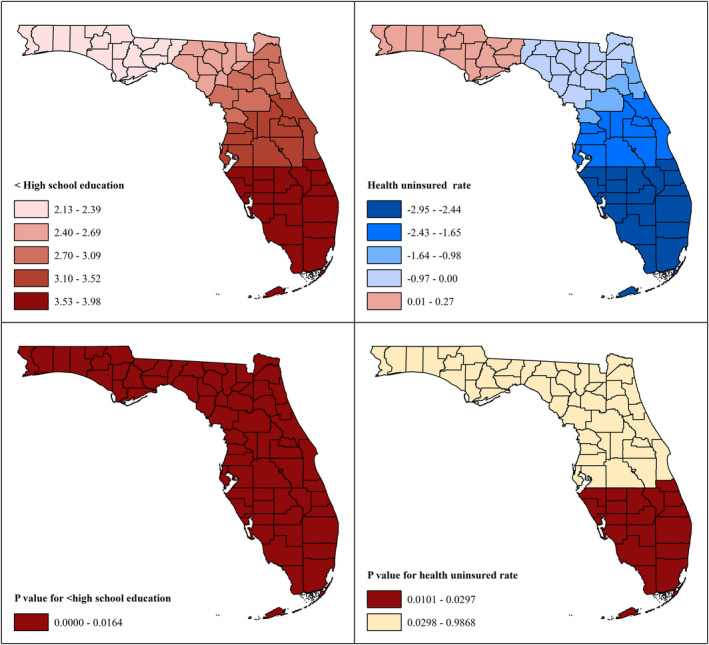
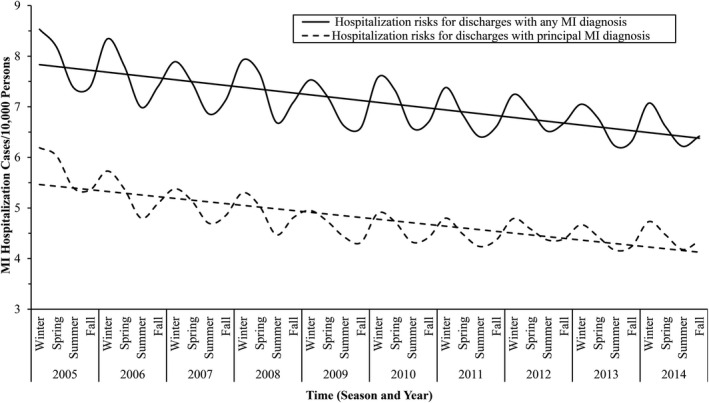
这是一项县级回顾性生态学研究。我们获得了 2005-2014 年佛罗里达州居民主要和次要 MI 住院的数据,并计算了年龄和性别调整后的 MI 住院风险。我们使用多变量负二项式模型确定 MI 住院风险的社会人口决定因素,并使用地理加权负二项式模型评估关联的强度是否因位置而异。共有 645935 例 MI 住院治疗(中位年龄 72 岁;58.1%为男性;73.9%为白人)。年龄和性别调整后的风险范围为 18.49 至 69.48 例/10000 人,在教育水平较低(风险比 [RR] = 1.033,<0.0001)和离婚率较高(RR,0.995;=0.018)的县中显著更高。然而,在农村(RR,0.996;<0.0001)、黑人(RR,1.026;=0.032)和未参保人群比例较高(RR,0.983;=0.040)的县中,风险显著降低。MI 住院风险与教育水平和未参保率的关联具有地理差异(非平稳性检验=0.001 和 0.043),在佛罗里达州南部最强(RR 对于<高中学历,1.036-1.041;RR 对于未参保率,0.971-0.976)。
黑人种族、离婚、农村居住、低教育水平和缺乏健康保险是 MI 住院风险的重要决定因素,但后两者的关联在佛罗里达州南部更强。因此,解决 MI 住院风险的干预措施需要优先考虑这些人群,并根据全球和地方模型的实证证据分配资源,以实现最大的效率和效果。