Gao Yuqian, Wang Yi-Ting, Chen Yongmei, Wang Hui, Young Denise, Shi Tujin, Song Yingjie, Schepmoes Athena A, Kuo Claire, Fillmore Thomas L, Qian Wei-Jun, Smith Richard D, Srivastava Sudhir, Kagan Jacob, Dobi Albert, Sesterhenn Isabell A, Rosner Inger L, Petrovics Gyorgy, Rodland Karin D, Srivastava Shiv, Cullen Jennifer, Liu Tao
Biological Sciences Division, Pacific Northwest National Laboratory, Richland, WA 99354, USA.
Henry M. Jackson Foundation for the Advancement of Military Medicine, Bethesda, MD 20817, USA.
Cancers (Basel). 2020 May 17;12(5):1268. doi: 10.3390/cancers12051268.
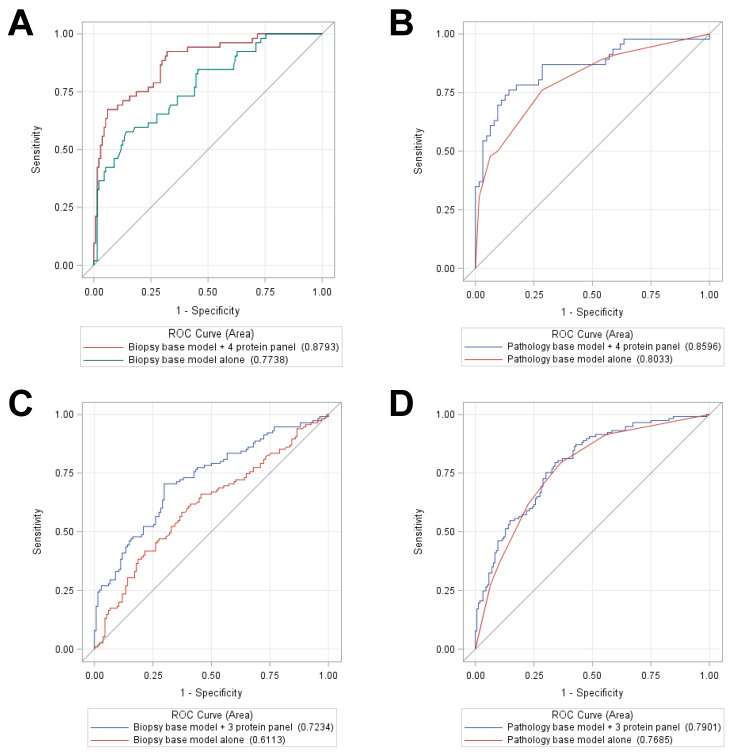
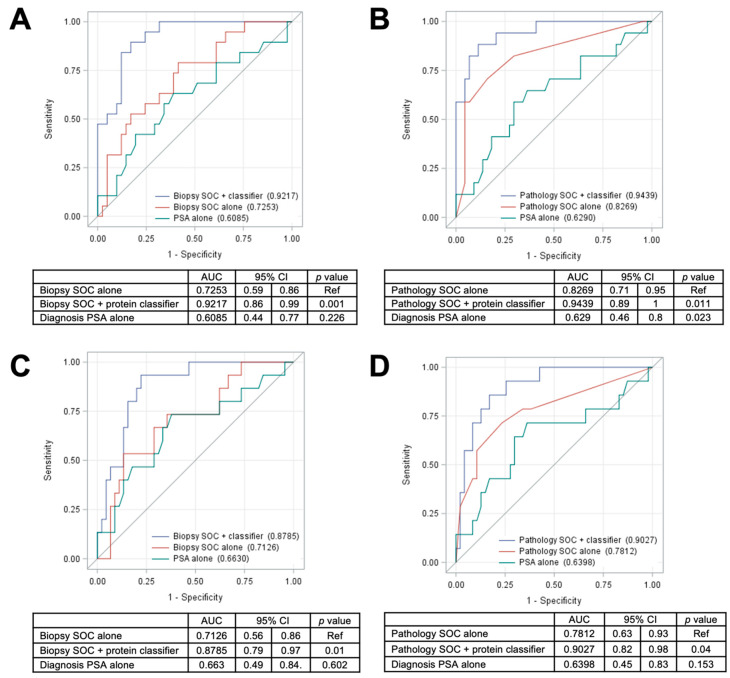
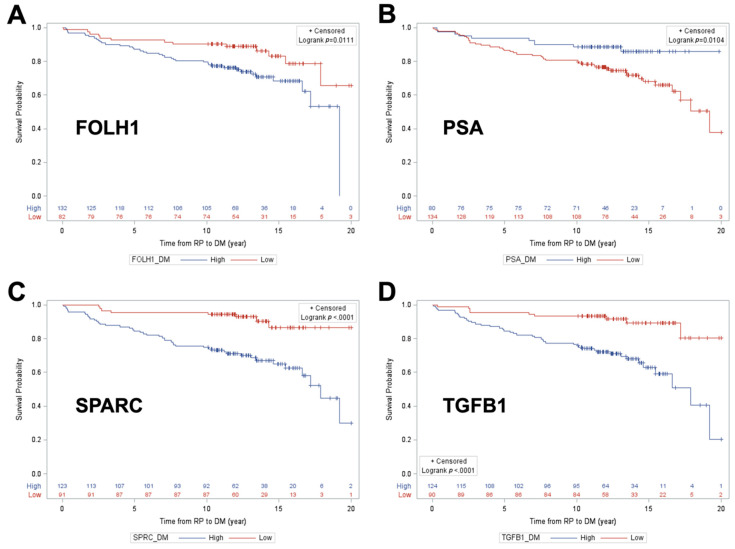
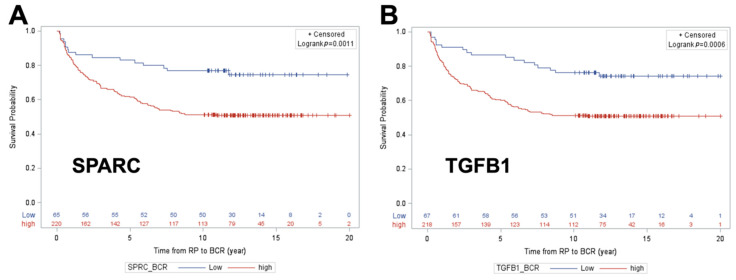
Although ~40% of screen-detected prostate cancers (PCa) are indolent, advanced-stage PCa is a lethal disease with 5-year survival rates around 29%. Identification of biomarkers for early detection of aggressive disease is a key challenge. Starting with 52 candidate biomarkers, selected from existing PCa genomics datasets and known PCa driver genes, we used targeted mass spectrometry to quantify proteins that significantly differed in primary tumors from PCa patients treated with radical prostatectomy (RP) across three study outcomes: (i) metastasis ≥1-year post-RP, (ii) biochemical recurrence ≥1-year post-RP, and (iii) no progression after ≥10 years post-RP. Sixteen proteins that differed significantly in an initial set of 105 samples were evaluated in the entire cohort (n = 338). A five-protein classifier which combined FOLH1, KLK3, TGFB1, SPARC, and CAMKK2 with existing clinical and pathological standard of care variables demonstrated significant improvement in predicting distant metastasis, achieving an area under the receiver-operating characteristic curve of 0.92 (0.86, 0.99, = 0.001) and a negative predictive value of 92% in the training/testing analysis. This classifier has the potential to stratify patients based on risk of aggressive, metastatic PCa that will require early intervention compared to low risk patients who could be managed through active surveillance.
尽管通过筛查发现的前列腺癌(PCa)中约40%为惰性癌,但晚期PCa是一种致命疾病,其5年生存率约为29%。识别用于早期检测侵袭性疾病的生物标志物是一项关键挑战。我们从现有的PCa基因组数据集和已知的PCa驱动基因中挑选出52个候选生物标志物,利用靶向质谱法定量分析了接受根治性前列腺切除术(RP)的PCa患者原发肿瘤中存在显著差异的蛋白质,这些差异与三个研究结果相关:(i)RP术后≥1年发生转移;(ii)RP术后≥1年出现生化复发;(iii)RP术后≥10年无疾病进展。在最初的105个样本中差异显著的16种蛋白质在整个队列(n = 338)中进行了评估。一种将FOLH1、KLK3、TGFB1、SPARC和CAMKK2与现有的临床和病理标准护理变量相结合的五蛋白分类器,在预测远处转移方面有显著改善,在训练/测试分析中,受试者操作特征曲线下面积为0.92(0.86,0.99,P = 0.001),阴性预测值为92%。与可通过主动监测管理的低风险患者相比,该分类器有潜力根据侵袭性转移性PCa的风险对患者进行分层,对于高风险患者可能需要早期干预。