Department of Radiation Oncology, University of Freiburg - Medical Center, Robert-Koch-Str. 3, 79106, Freiburg, Germany.
German Cancer Consortium (DKTK) Partner Site Freiburg, German Cancer Research Center (dkfz), Neuenheimer Feld 280, 69120, Heidelberg, Germany.
Radiat Oncol. 2020 May 19;15(1):113. doi: 10.1186/s13014-020-01563-x.
The number of nonagenarian cancer patients (≥ 90 years) is continuously increasing, and radiotherapy is performed in a relevant proportion of patients, as surgery and chemotherapy are often not feasible for these patients. However, the evidence regarding the feasibility and treatment outcomes after radiotherapy for this patient group is very limited.
All nonagenarian patients receiving (chemo) radiotherapy between 2009 and 2019 at the University of Freiburg - Medical Center were analyzed for patterns of care, overall survival (OS) and therapy-associated toxicities according to the Common Terminology Criteria for Adverse Events. Uni- and multivariate Cox regression analyses were conducted to assess the influence of patient- and treatment-related factors on patient outcomes.
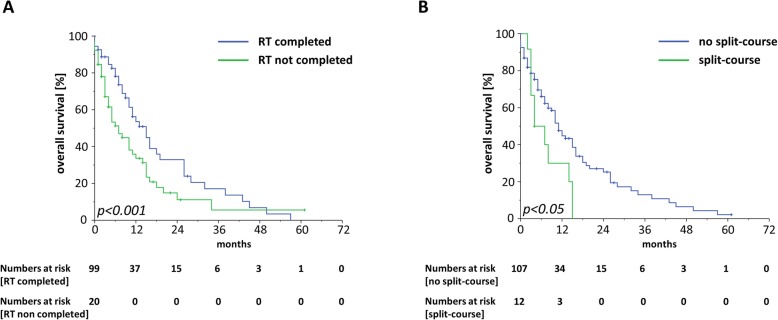
One hundred nineteen patients with a total of 137 irradiated lesions were included in this analysis. After a median follow-up of 27 months, median OS was 10 months with a 3-year OS amounting to 11.1%. Univariate analyses demonstrated that a reduced performance status (HR = 1.56, 95% CI 1.00-2.45, p < 0.05), a higher burden of comorbidities (HR = 2.00, 95% CI 1.00-4.10, p < 0.05) and higher UICC tumor stages (HR = 2.21, 95% CI 1.14-4.26, p < 0.05) were associated with impaired survival rates. Split-course treatments (HR = 2.05, 95% CI 1.07-3.94, p < 0.05), non-completion of radiotherapy (HR = 7.17, 95% CI 3.88-13.26, p < 0.001) and palliative treatments (HR = 2.84, 95% CI 1.68-4.81, p < 0.05) were found to result in significantly reduced OS. In the multivariate analysis, split-course concepts (HR = 2.21, 95% CI 1.10-4.37, p < 0.05) and palliative treatments (HR = 3.19, 95% CI 1.77-5.75, p < 0.001) significantly deteriorated outcomes, while impaired ECOG status (HR = 1.49, 95% CI 0.91-2.43, p = 0.11) did not. The vast majority of patients reported either no (n = 40; 33.6%) or grade 1-2 acute toxicities (n = 66; 55.5%), and only very few higher-grade toxicities were observed in our study.
Radiotherapy for nonagenarian patients is generally feasible and associated with a low toxicity profile. Given the relatively poor OS rates and the importance of the quality of life for this patient group, individualized treatment regimens including hypofractionation concepts should be considered.
90 岁以上的非老年癌症患者(≥90 岁)的数量不断增加,相当一部分患者接受放疗,因为手术和化疗对这些患者往往不可行。然而,关于该患者组接受放疗后的可行性和治疗结果的证据非常有限。
对 2009 年至 2019 年期间在弗赖堡大学医疗中心接受(化疗)放疗的所有 90 岁以上患者的治疗模式、总生存率(OS)和根据常见不良事件术语标准评估的治疗相关毒性进行分析。采用单因素和多因素 Cox 回归分析评估患者和治疗相关因素对患者结局的影响。
本分析共纳入 119 例患者,共 137 个放疗病灶。中位随访 27 个月后,中位 OS 为 10 个月,3 年 OS 率为 11.1%。单因素分析表明,体力状态下降(HR=1.56,95%CI 1.00-2.45,p<0.05)、合并症负担增加(HR=2.00,95%CI 1.00-4.10,p<0.05)和更高的 UICC 肿瘤分期(HR=2.21,95%CI 1.14-4.26,p<0.05)与生存率下降相关。分割疗程治疗(HR=2.05,95%CI 1.07-3.94,p<0.05)、放疗未完成(HR=7.17,95%CI 3.88-13.26,p<0.001)和姑息治疗(HR=2.84,95%CI 1.68-4.81,p<0.05)与显著降低的 OS 相关。在多因素分析中,分割疗程治疗(HR=2.21,95%CI 1.10-4.37,p<0.05)和姑息治疗(HR=3.19,95%CI 1.77-5.75,p<0.001)显著恶化了结果,而体力状态下降(HR=1.49,95%CI 0.91-2.43,p=0.11)没有。绝大多数患者报告无(n=40;33.6%)或 1-2 级急性毒性(n=66;55.5%),研究中仅观察到少数较高等级的毒性。
对于 90 岁以上的患者,放疗通常是可行的,且具有较低的毒性特征。鉴于该患者组的 OS 率相对较差,以及生活质量对该患者组的重要性,应考虑个体化治疗方案,包括分割治疗概念。