Department I of Internal Medicine, Center for Integrated Oncology Aachen Bonn Cologne Duesseldorf, Lung Cancer Group, University of Cologne, Cologne, Germany.
Onkologische Praxis Moers, Moers, Germany.
Cancer Med. 2020 Jul;9(14):4991-5007. doi: 10.1002/cam4.3131. Epub 2020 May 21.
Treatment of patients with solid tumors and KRAS mutations remains disappointing. One option is the combined inhibition of pathways involved in RAF-MEK-ERK and PI3K-AKT-mTOR.
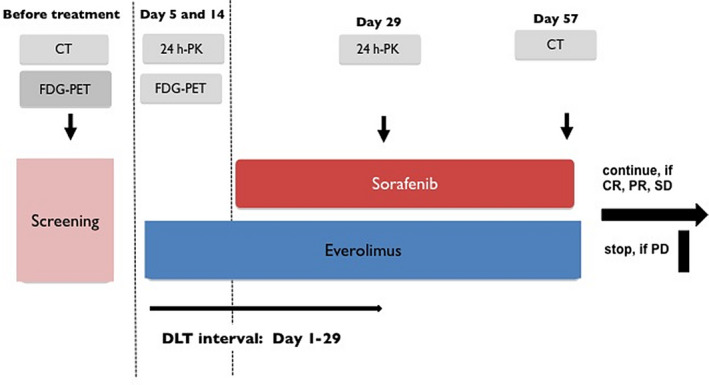
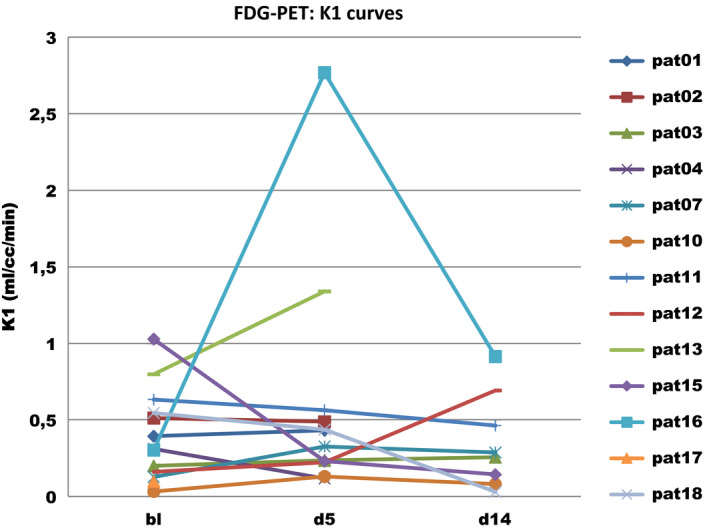
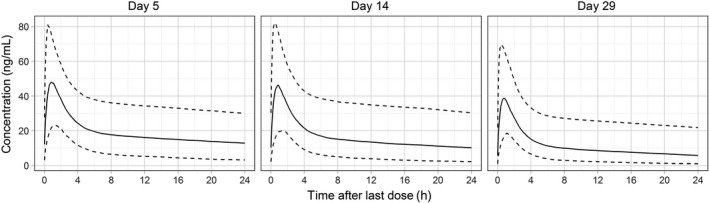
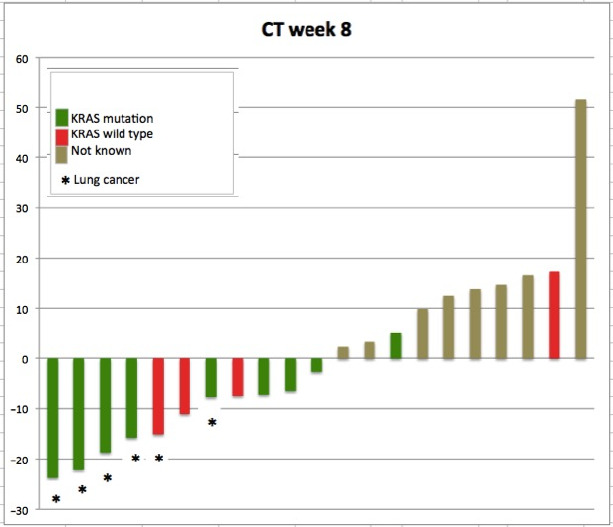
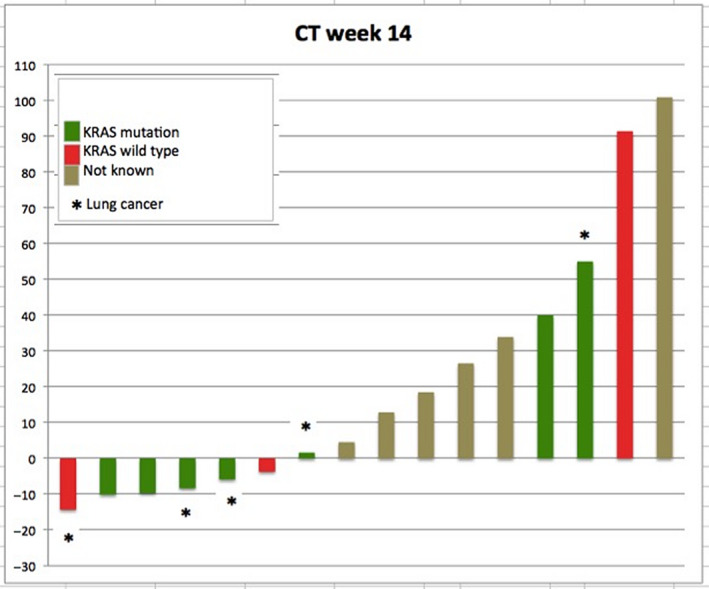
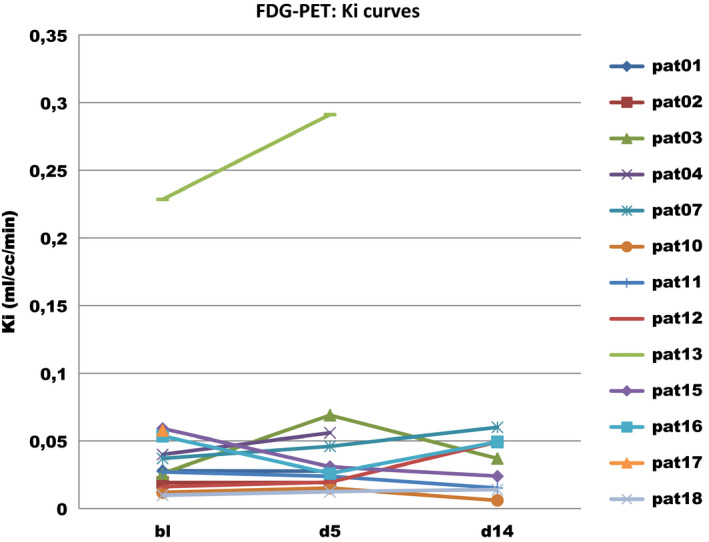
Patients with relapsed solid tumors were treated with escalating doses of everolimus (E) 2.5-10.0 mg/d in a 14-day run-in phase followed by combination therapy with sorafenib (S) 800 mg/d from day 15. KRAS mutational status was assessed retrospectively in the escalation phase. Extension phase included KRAS-mutated non-small-cell lung cancer (NSCLC) only. Pharmacokinetic analyses were accompanied by pharmacodynamics assessment of E by FDG-PET. Efficacy was assessed by CT scans every 6 weeks of combination.
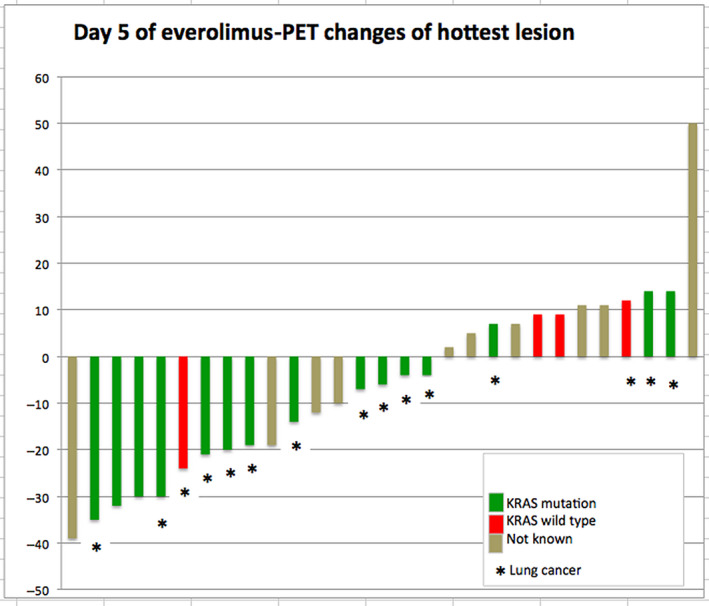
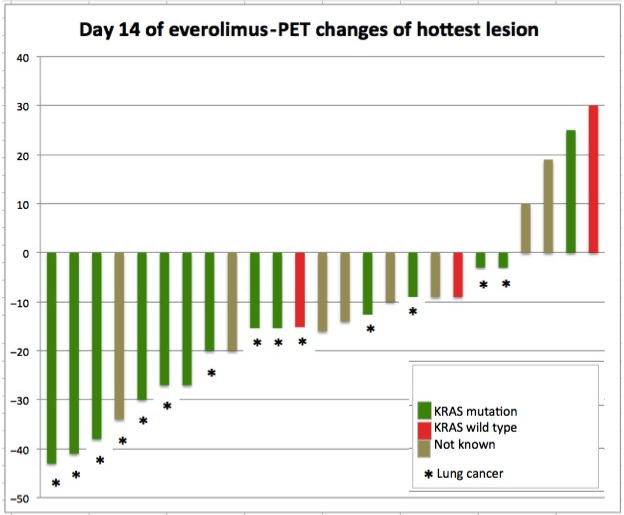
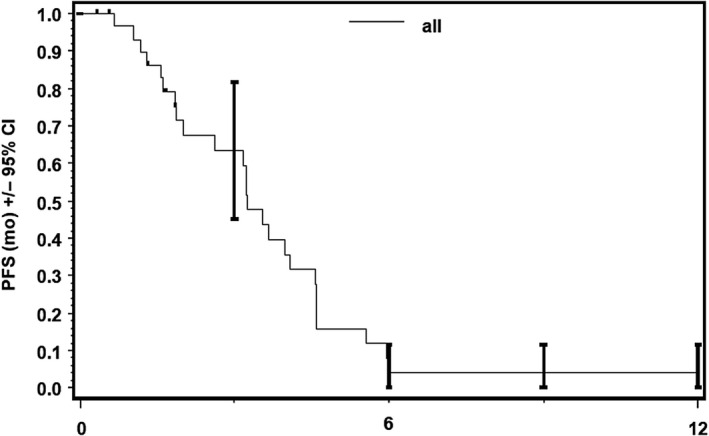
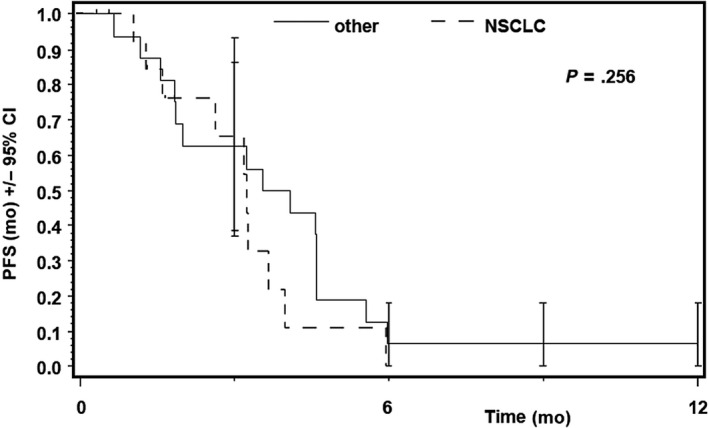
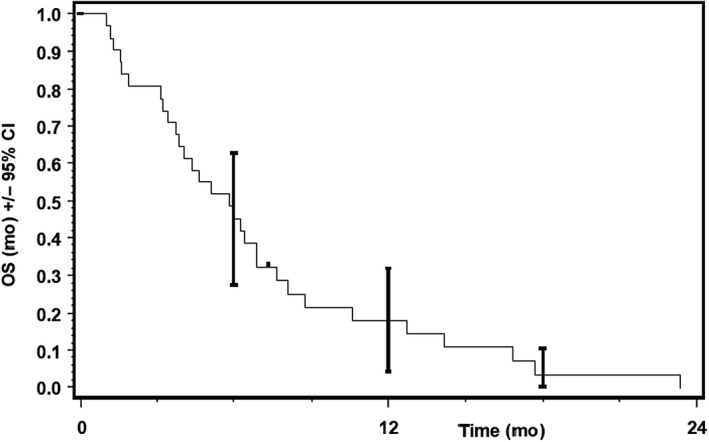
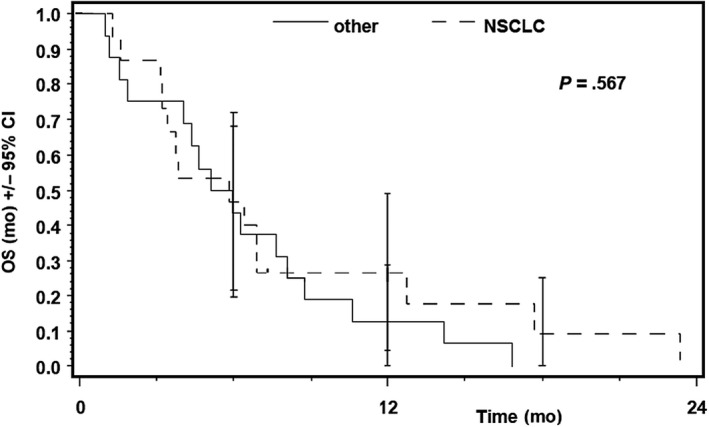
Of 31 evaluable patients, 15 had KRAS mutation, 4 patients were negative for KRAS mutation, and the KRAS status remained unknown in 12 patients. Dose-limiting toxicity (DLT) was not reached. The maximum tolerated dose (MTD) was defined as 7.5 mg/d E + 800 mg/d S due to toxicities at previous dose level (10 mg/d E + 800 mg/d S) including leucopenia/thrombopenia III° and pneumonia III° occurring after the DLT interval. The metabolic response rate in FDG-PET was 17% on day 5 and 20% on day 14. No patient reached partial response in CT scan. Median progression free survival (PFS) and overall survival (OS) were 3.25 and 5.85 months, respectively.
Treatment of patients with relapsed solid tumors with 7.5 mg/d E and 800 mg/d S is safe and feasible. Early metabolic response in FDG-PET was not confirmed in CT scan several weeks later. The combination of S and E is obviously not sufficient to induce durable responses in patients with KRAS-mutant solid tumors.
治疗携带 KRAS 突变的实体瘤患者的效果仍令人失望。一种选择是联合抑制 RAF-MEK-ERK 和 PI3K-AKT-mTOR 通路。
在为期 14 天的爬坡期内,患者接受递增剂量的依维莫司(E)2.5-10.0mg/d,随后从第 15 天开始联合索拉非尼(S)800mg/d 进行治疗。在爬坡期内对 KRAS 突变状态进行回顾性评估。扩展期仅包括 KRAS 突变型非小细胞肺癌(NSCLC)。伴随依维莫司的药效动力学评估,同时进行了氟脱氧葡萄糖正电子发射断层扫描(FDG-PET)的药代动力学分析。每 6 周通过 CT 扫描评估联合治疗的疗效。
在 31 名可评估的患者中,15 名患者存在 KRAS 突变,4 名患者 KRAS 突变阴性,12 名患者的 KRAS 状态未知。未达到剂量限制毒性(DLT)。由于先前剂量水平(10mg/d E+800mg/d S)的毒性,包括 DLT 间隔后发生的 III°白细胞减少/血小板减少和 III°肺炎,将最大耐受剂量(MTD)定义为 7.5mg/d E+800mg/d S。FDG-PET 在第 5 天的代谢缓解率为 17%,第 14 天为 20%。在 CT 扫描中没有患者达到部分缓解。中位无进展生存期(PFS)和总生存期(OS)分别为 3.25 个月和 5.85 个月。
在复发的实体瘤患者中,每天给予 7.5mg/d E 和 800mg/d S 的治疗是安全可行的。几周后 CT 扫描并未确认 FDG-PET 早期代谢反应。S 和 E 的联合治疗显然不足以诱导 KRAS 突变型实体瘤患者的持久缓解。