Yayli Gizem, Tokofsky Alexa, Nayar Utthara
Department of Biochemistry and Molecular Biology, Bloomberg School of Public Health, Johns Hopkins University, Baltimore, MD, United States.
Oncology, Sidney Kimmel Comprehensive Cancer Center, School of Medicine, Johns Hopkins University, Baltimore, MD, United States.
Front Oncol. 2024 Nov 22;14:1461190. doi: 10.3389/fonc.2024.1461190. eCollection 2024.
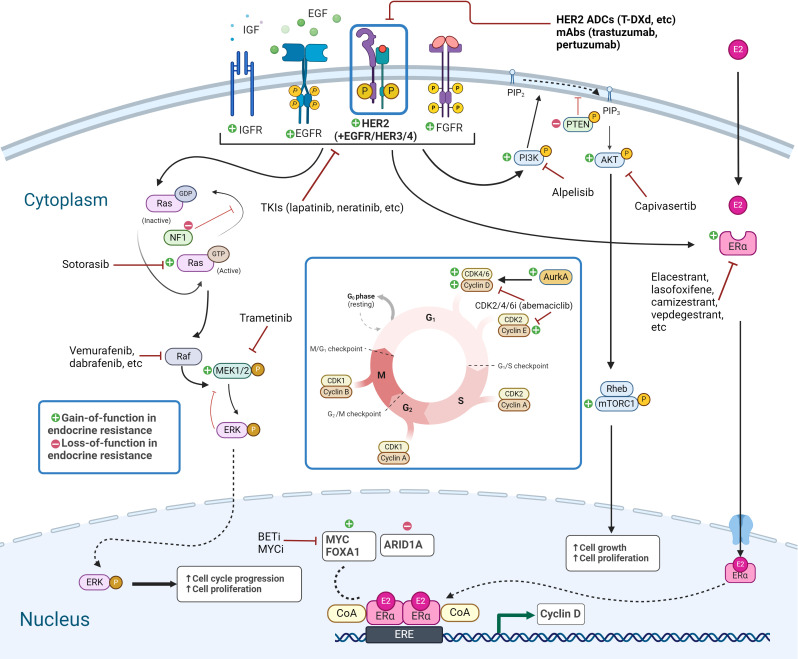
Since its introduction in the 1970s, endocrine therapy that targets the estrogen receptor alpha (ERα) signaling pathway has had tremendous success in the clinic in estrogen receptor positive (ER+) breast cancer. However, resistance to endocrine therapy eventually develops in virtually all patients with metastatic disease. Endocrine resistance is a primary unaddressed medical need for ER+ metastatic breast cancer patients. It has been shown that tumors become resistant through various mechanisms, converging on the acquisition of genetic alterations of ER, components of the MAP kinase pathway, or transcription factors (TFs). For instance, mutations in the human epidermal growth factor receptor-2 (HER2) lead to complete resistance to all current endocrine therapies including aromatase inhibitors, selective estrogen receptor modulators, and selective estrogen receptor degraders, as well as cross-resistance to CDK4/6 inhibitors (CDK4/6is). Emerging evidence points to an intriguing connection between endocrine-resistant tumors and the HER2-low subtype. Specifically, recent studies and our analysis of a publicly available breast cancer dataset both indicate that metastatic ER+ breast cancer with endocrine resistance conferred through acquired genetic alterations can often be classified as HER2-low rather than HER2-0/HER2-negative. Limited data suggest that acquired endocrine resistance can also be accompanied by a subtype switch. Therefore, we suggest that there is an underappreciated association between the HER2-low subtype and endocrine resistance. In this perspective piece, we explore the evidence linking the HER2-low subtype with the various pathways to endocrine resistance and suggest that there are signaling networks in HER2-low tumors that intersect endocrine resistance and can be effectively targeted.
自20世纪70年代引入以来,针对雌激素受体α(ERα)信号通路的内分泌疗法在雌激素受体阳性(ER+)乳腺癌的临床治疗中取得了巨大成功。然而,几乎所有转移性疾病患者最终都会对内分泌疗法产生耐药性。内分泌耐药是ER+转移性乳腺癌患者尚未得到解决的主要医疗需求。已经表明,肿瘤通过多种机制产生耐药性,最终导致ER、丝裂原活化蛋白激酶(MAP)激酶途径的组成部分或转录因子(TFs)发生基因改变。例如,人表皮生长因子受体2(HER2)的突变会导致对所有当前内分泌疗法(包括芳香化酶抑制剂、选择性雌激素受体调节剂和选择性雌激素受体降解剂)产生完全耐药性,以及对细胞周期蛋白依赖性激酶4/6抑制剂(CDK4/6is)产生交叉耐药性。新出现的证据表明,内分泌耐药肿瘤与HER2低表达亚型之间存在着有趣的联系。具体而言,最近的研究以及我们对一个公开可用的乳腺癌数据集的分析均表明,通过获得性基因改变产生内分泌耐药性的转移性ER+乳腺癌通常可归类为HER2低表达而非HER2零表达/HER2阴性。有限的数据表明,获得性内分泌耐药也可能伴随着亚型转换。因此,我们认为HER2低表达亚型与内分泌耐药之间的关联尚未得到充分认识。在这篇观点文章中,我们探讨了将HER2低表达亚型与内分泌耐药的各种途径联系起来的证据,并表明HER2低表达肿瘤中存在与内分泌耐药相交且可有效靶向的信号网络。