Keller Kira, Jacobi Barbara, Jabal Mahmoud, Stavrou Gregor Alexander
Department of General, Visceral, Thoracic, and Oncologic Surgery, Klinikum Saarbrücken, Germany.
Department of General, Visceral, Thoracic, and Oncologic Surgery, Klinikum Saarbrücken, Germany.
Int J Surg Case Rep. 2020;71:50-53. doi: 10.1016/j.ijscr.2020.04.094. Epub 2020 May 13.
Leiomyosarcomas are rare and heterogeneous group of tumors that account for less than 1% of adult malignancies. More than 50% of all vascular leiomyosarcomas occur in the lower part of vena cava. Since the first description of Perl and Virchow in 1871, only approximately 450 cases have been reported in literature.
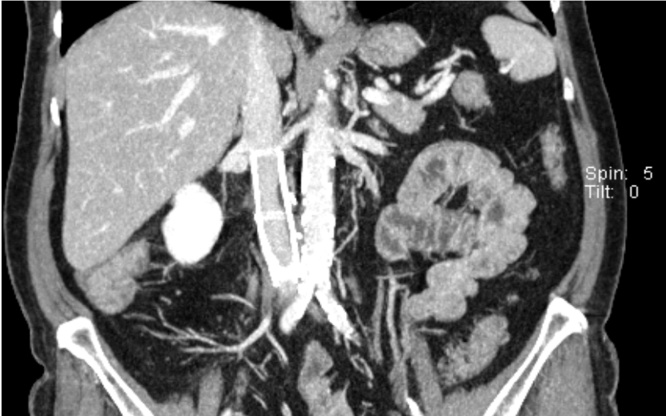
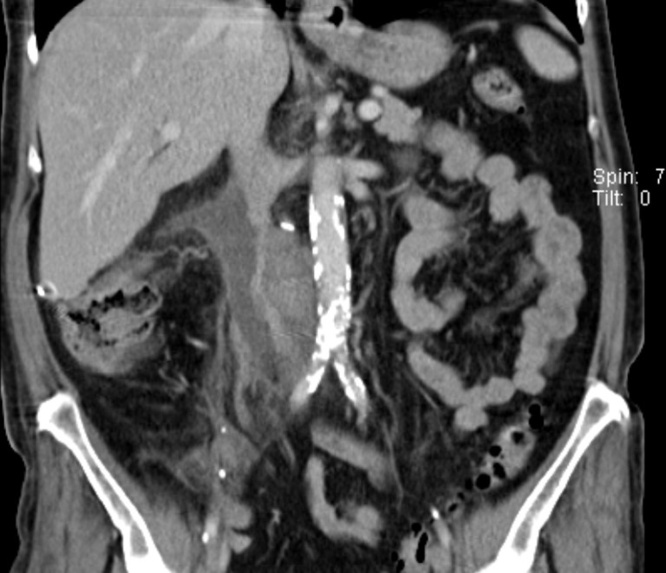
The patient presented due to abdominal pain and weight loss. Based on the imaging evaluations a retroduodenal tumor with compression of the inferior vena cava was observed. In the explorative laparotomy a leiomyosarcoma originating from the inferior vena cava was identified. Considering the extensive intramural and intraluminal tumor manifestation, the patient underwent a segmental resection of the vena cava. Reconstruction was achieved by implanting a polytetrafluoroethylene (PTFE) prosthesis. Postoperatively a stenosis developed due to a pericaval haematoma with consecutive compression of the prosthesis. An angiographic implantation of a stent was successfully performed. In the 24-month follow-up, the patient is free of symptoms and tumors.
Leiomyosarcomas of the vena cava are classified anatomically according to their relationship to the liver and renal vessels. The clinical symptoms depend on the affected segment. The therapy of choice is radical en bloc tumor resection. After resection, the options for reconstruction include placement of a synthetic graft, primary repair and patch repair.
Due to a variety of topographic and tumor biological sarcoma manifestations, no standard has been established for the resection of this entity. The extent of resection should be planned individually.
平滑肌肉瘤是一种罕见且异质性的肿瘤群体,占成人恶性肿瘤的比例不到1%。所有血管平滑肌肉瘤中超过50%发生在下腔静脉下部。自1871年珀尔(Perl)和魏尔啸(Virchow)首次描述以来,文献中仅报道了约450例病例。
患者因腹痛和体重减轻就诊。基于影像学评估,观察到十二指肠后肿瘤压迫下腔静脉。在剖腹探查术中,发现起源于下腔静脉的平滑肌肉瘤。考虑到肿瘤广泛的壁内和腔内表现,患者接受了下腔静脉节段性切除。通过植入聚四氟乙烯(PTFE)假体实现重建。术后由于腔静脉周围血肿导致假体受压,出现了狭窄。成功进行了支架血管造影植入术。在24个月的随访中,患者无症状且无肿瘤。
腔静脉平滑肌肉瘤根据其与肝血管和肾血管的关系进行解剖学分类。临床症状取决于受累节段。首选治疗方法是根治性整块肿瘤切除。切除后,重建选择包括放置人工血管移植物、一期修复和补片修复。
由于肉瘤在地形学和肿瘤生物学方面表现多样,对于该实体的切除尚未建立标准。切除范围应个体化规划。