British Heart Foundation Centre of Excellence and National Institute for Health Research Biomedical Research Centre at the School of Cardiovascular Medicine and Sciences, Kings College London, London, United Kingdom.
School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom.
J Am Coll Cardiol. 2020 May 26;75(20):2538-2549. doi: 10.1016/j.jacc.2020.03.051.
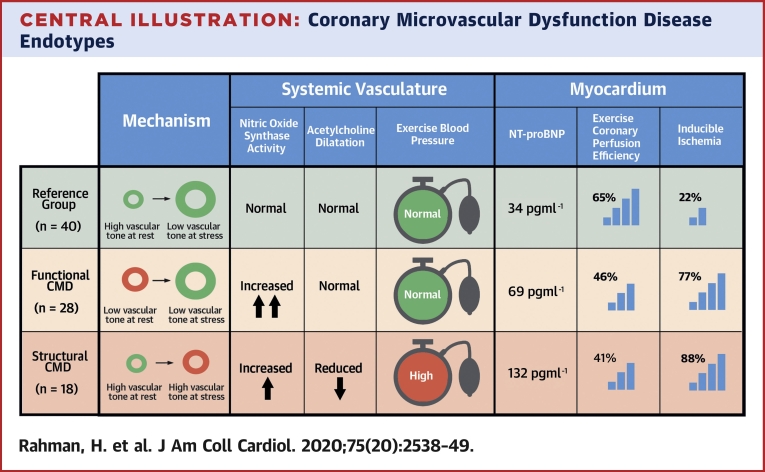
Coronary microvascular dysfunction (CMD) is defined by diminished flow reserve. Functional and structural CMD endotypes have recently been described, with normal and elevated minimal microvascular resistance, respectively.
This study determined the mechanism of altered resting and maximal flow in CMD endotypes.
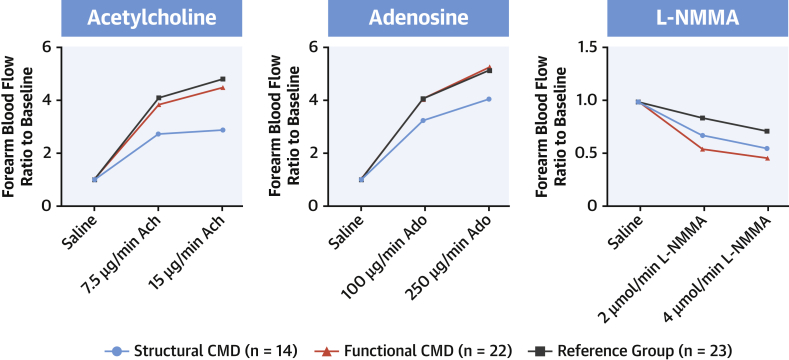
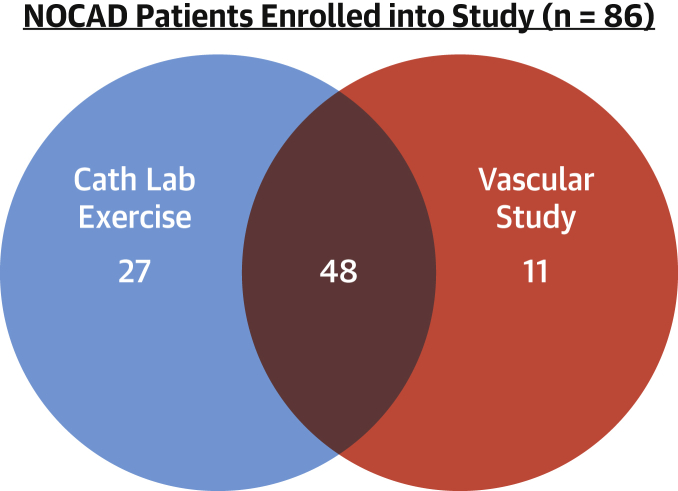
A total of 86 patients with angina but no obstructive coronary disease underwent coronary pressure and flow measurement during rest, exercise, and adenosine-mediated hyperemia and were classified as the reference group or as patients with CMD by a coronary flow reserve threshold of 2.5; functional or structural endotypes were distinguished by a hyperemic microvascular resistance threshold of 2.5 mm Hg/cm/s. Endothelial function was assessed by forearm blood flow (FBF) response to acetylcholine, and nitric oxide synthase (NOS) activity was defined as the inverse of FBF reserve to N-monomethyl-L-arginine.
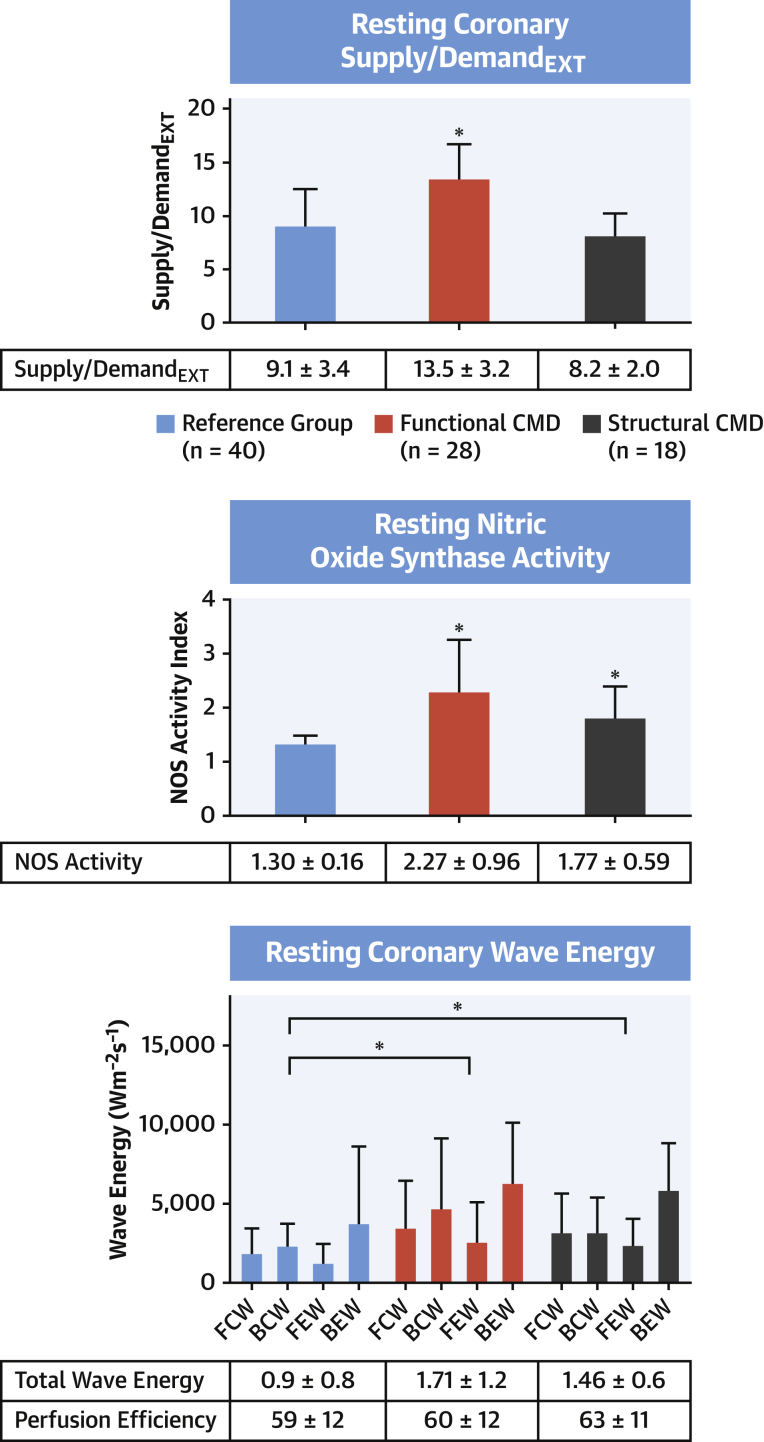
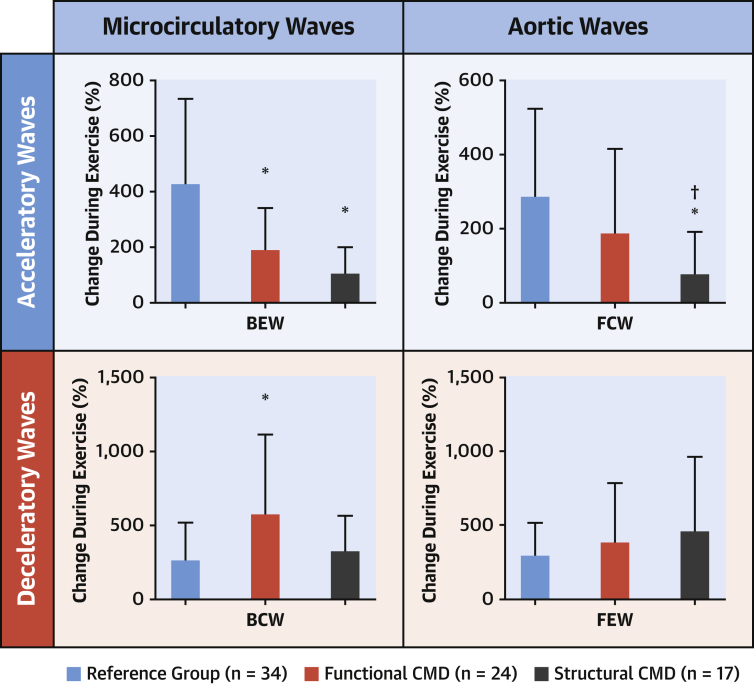
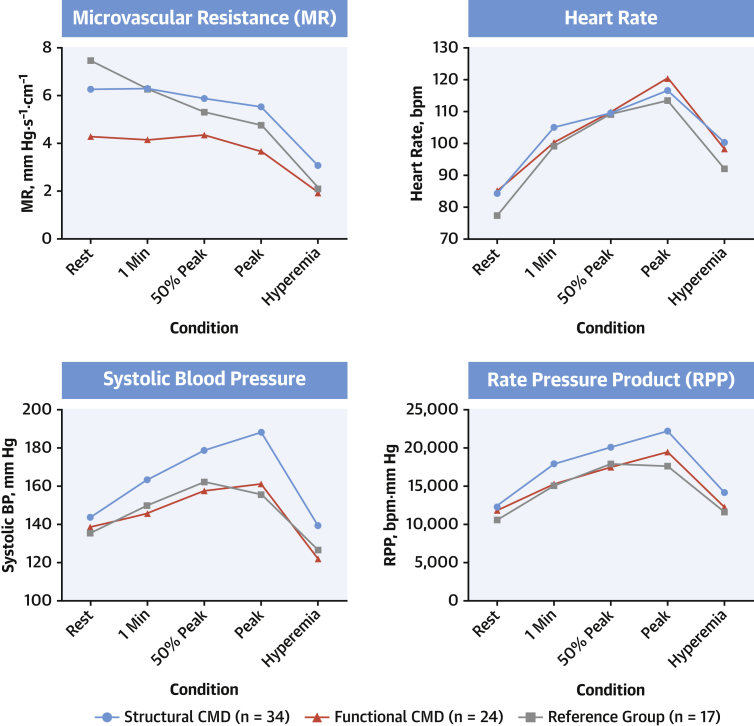
Of the 86 patients, 46 had CMD (28 functional, 18 structural), and 40 patients formed the reference group. Resting coronary blood flow (CBF) (24.6 ± 2.0 cm/s vs. 16.6 ± 3.9 cm/s vs. 15.1 ± 4.7 cm/s; p < 0.001) and NOS activity (2.27 ± 0.96 vs. 1.77 ± 0.59 vs. 1.30 ± 0.16; p < 0.001) were higher in the functional group compared with the structural CMD and reference groups, respectively. The structural group had lower acetylcholine FBF augmentation than the functional or reference group (2.1 ± 1.8 vs. 4.1 ± 1.7 vs. 4.5 ± 2.0; p < 0.001). On exercise, oxygen demand was highest (rate-pressure product: 22,157 ± 5,497 beats/min/mm Hg vs. 19,519 ± 4,653 beats/min/mm Hg vs. 17,530 ± 4,678 beats/min/mm Hg; p = 0.004), but peak CBF was lowest in patients with structural CMD compared with the functional and reference groups.
Functional CMD is characterized by elevated resting flow that is linked to enhanced NOS activity. Patients with structural CMD have endothelial dysfunction, which leads to diminished peak CBF augmentation and increased demand during exercise. The value of pathophysiologically stratified therapy warrants investigation.
冠状动脉微血管功能障碍(CMD)的定义是血流储备减少。最近已经描述了功能性和结构性 CMD 亚型,分别具有正常和升高的最小微血管阻力。
本研究旨在确定 CMD 亚型中静息和最大血流改变的机制。
共有 86 名心绞痛但无阻塞性冠状动脉疾病的患者在静息、运动和腺苷介导的充血期间接受冠状动脉压力和流量测量,并通过冠状动脉血流储备阈值 2.5 分为参考组或 CMD 患者;通过 2.5mmHg/cm/s 的充血性微血管阻力阈值区分功能性或结构性亚型。通过乙酰胆碱引起的前臂血流(FBF)反应评估内皮功能,并且一氧化氮合酶(NOS)活性被定义为 N-单甲基-L-精氨酸对 FBF 储备的倒数。
在 86 名患者中,46 名患有 CMD(28 名功能性,18 名结构性),40 名患者形成参考组。静息冠状动脉血流(CBF)(24.6±2.0cm/s 比 16.6±3.9cm/s 比 15.1±4.7cm/s;p<0.001)和 NOS 活性(2.27±0.96 比 1.77±0.59 比 1.30±0.16;p<0.001)在功能性组分别高于结构性 CMD 和参考组。结构性组的乙酰胆碱 FBF 增强低于功能性或参考组(2.1±1.8 比 4.1±1.7 比 4.5±2.0;p<0.001)。在运动期间,需氧量最高(心率-血压乘积:22157±5497 次/分/mmHg 比 19519±4653 次/分/mmHg 比 17530±4678 次/分/mmHg;p=0.004),但与功能性和参考组相比,结构性 CMD 患者的峰值 CBF 最低。
功能性 CMD 的特征是静息时的流量增加,这与 NOS 活性增强有关。结构性 CMD 患者存在内皮功能障碍,导致峰值 CBF 增强减少和运动时需求增加。分层治疗的价值值得进一步研究。