From The British Heart Foundation Centre of Research Excellence, Schools of Cardiovascular Medicine & Sciences (H.R., M.R., M.L., B.M., H.M., H.E., B.C., M.M., A.W., D.P.), King's College London, United Kingdom.
Biomedical Engineering & Imaging Sciences (A.C., C.S.), King's College London, United Kingdom.
Circulation. 2019 Nov 26;140(22):1805-1816. doi: 10.1161/CIRCULATIONAHA.119.041595. Epub 2019 Nov 11.
Coronary microvascular dysfunction (MVD) is defined by impaired flow augmentation in response to a pharmacological vasodilator in the presence of nonobstructive coronary artery disease. It is unknown whether diminished coronary vasodilator response correlates with abnormal exercise physiology or inducible myocardial ischemia.
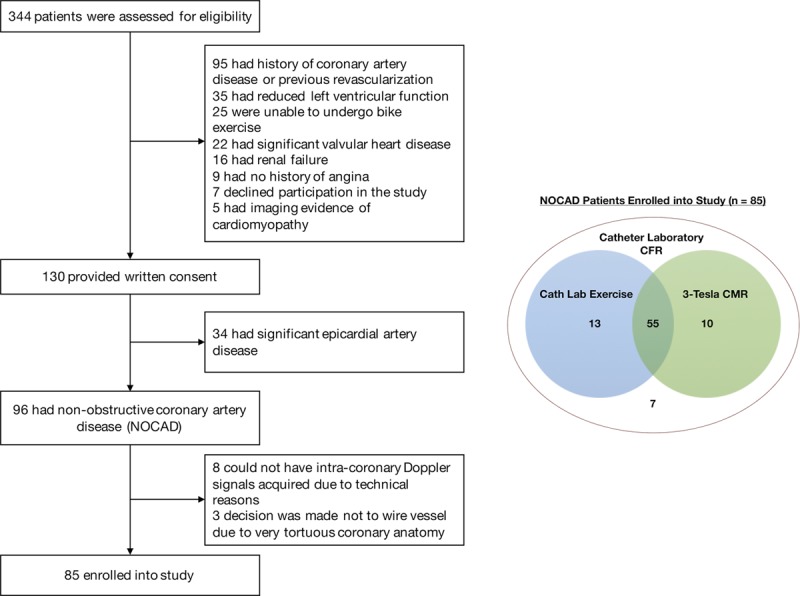
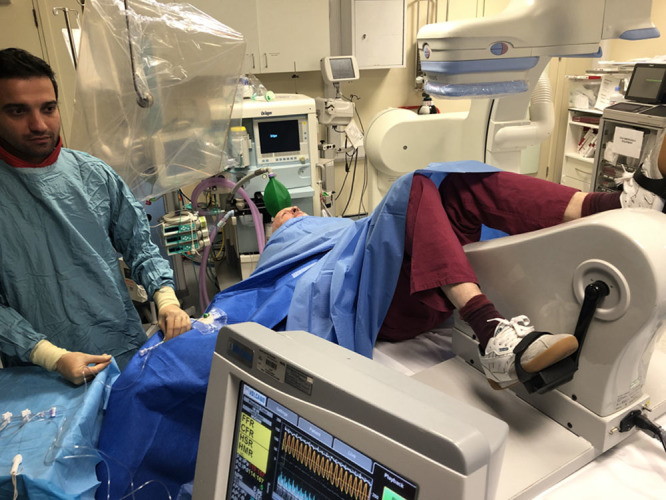
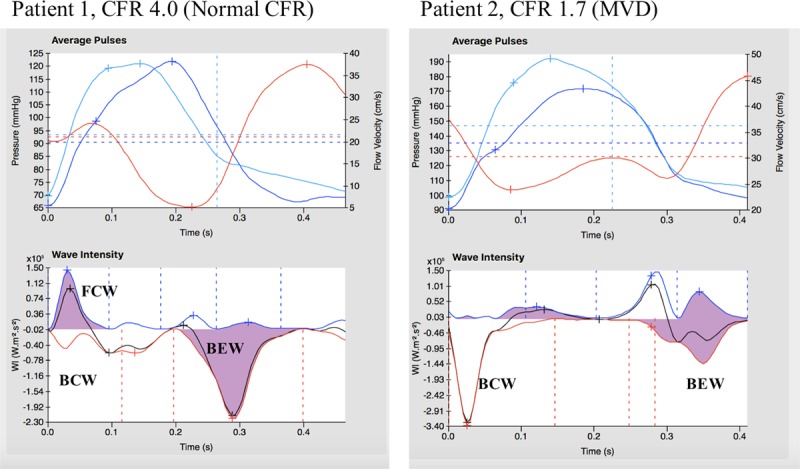
Patients with angina and nonobstructive coronary artery disease had simultaneous coronary pressure and flow velocity measured using a dual sensor-tipped guidewire during rest, supine bicycle exercise, and adenosine-mediated hyperemia. Microvascular resistance (MR) was calculated as coronary pressure divided by flow velocity. Wave intensity analysis quantified the proportion of accelerating wave energy (perfusion efficiency). Global myocardial blood flow and subendocardial:subepicardial perfusion ratio were quantified using 3-Tesla cardiac magnetic resonance imaging during hyperemia and rest; inducible ischemia was defined as hyperemic subendocardial:subepicardial perfusion ratio <1.0. Patients were classified as having MVD if coronary flow reserve <2.5 and controls if coronary flow reserve ≥2.5, with researchers blinded to the classification.
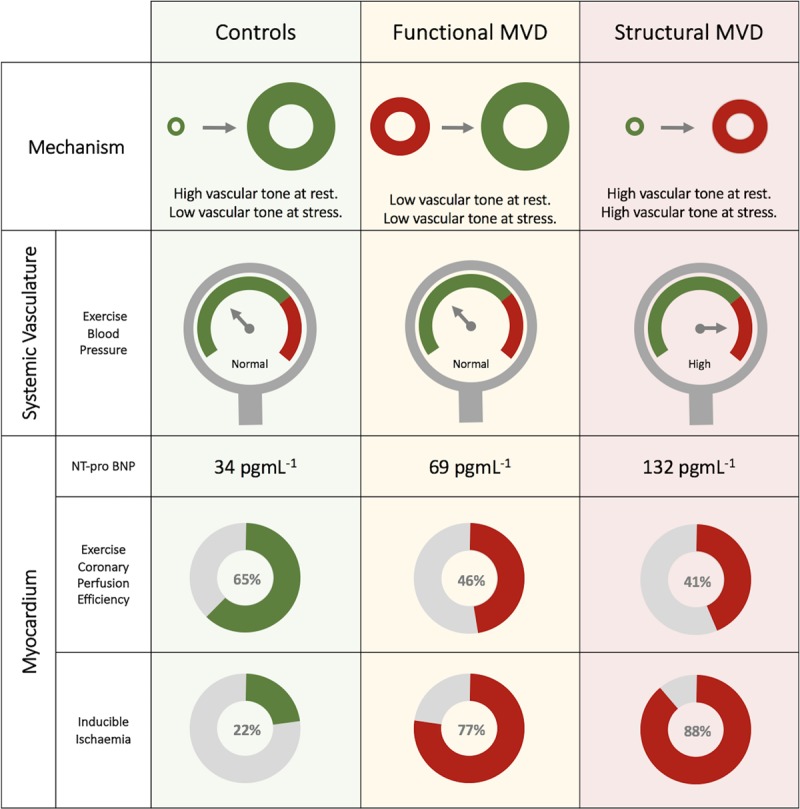
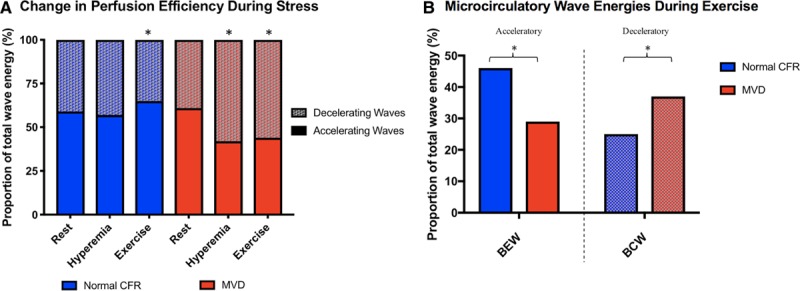
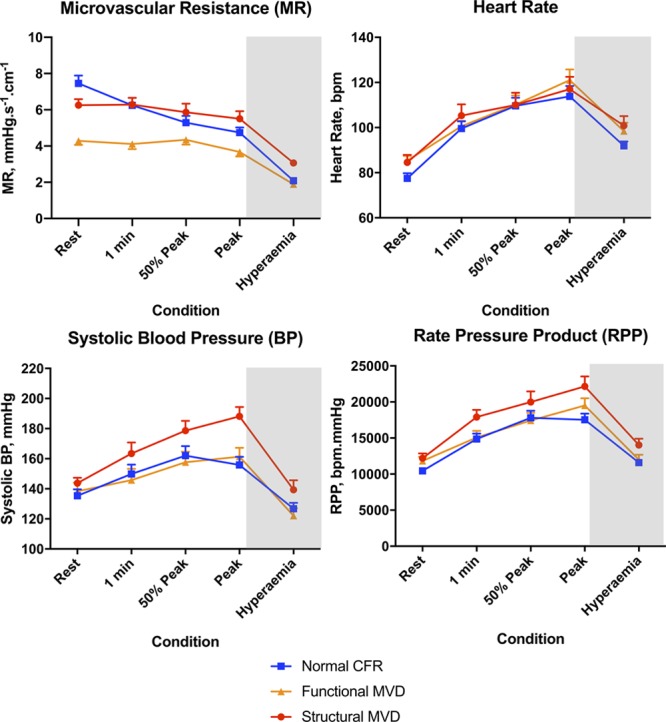
Eighty-five patients were enrolled (78% female, 57±10 years), 45 (53%) were classified as having MVD. Of the MVD group, 82% had inducible ischemia compared with 22% of controls (<0.001); global myocardial perfusion reserve was 2.01±0.41 and 2.68±0.49 (<0.001). In controls, coronary perfusion efficiency improved from rest to exercise and was unchanged during hyperemia (59±11% vs 65±14% vs 57±18%; =0.02 and =0.14). In contrast, perfusion efficiency decreased during both forms of stress in MVD (61±12 vs 44±10 vs 42±11%; both <0.001). Among patients with a coronary flow reserve <2.5, 62% had functional MVD, with normal minimal MR (hyperemic MR<2.5 mmHg/cm/s), and 38% had structural MVD with elevated hyperemic MR. Resting MR was lower in those with functional MVD (4.2±1.0 mmHg/cm/s) than in those with structural MVD (6.9±1.7 mmHg/cm/s) or controls (7.3±2.2 mmHg/cm/s; both <0.001). During exercise, the structural group had a higher systolic blood pressure (188±25 mmHg) than did those with functional MVD (161±27 mmHg; =0.004) and controls (156±30 mmHg; <0.001). Functional and structural MVD had similar stress myocardial perfusion and exercise perfusion efficiency values.
In patients with angina and nonobstructive coronary artery disease, diminished coronary flow reserve characterizes a cohort with inducible ischemia and a maladaptive physiological response to exercise. We have identified 2 endotypes of MVD with distinctive systemic vascular responses to exercise; whether endotypes have a different prognosis or require different treatments merits further investigation.
冠状动脉微血管功能障碍(MVD)定义为在存在非阻塞性冠状动脉疾病的情况下,对药物引起的血管扩张剂的血流增强反应受损。目前尚不清楚冠状动脉舒张反应的减弱是否与异常运动生理学或可诱导性心肌缺血有关。
患有心绞痛和非阻塞性冠状动脉疾病的患者在休息、仰卧位自行车运动和腺苷介导的充血期间使用带有双传感器尖端的导丝同时测量冠状动脉压力和血流速度。微血管阻力(MR)定义为冠状动脉压力除以血流速度。波强度分析量化了加速波能量的比例(灌注效率)。在充血和休息期间使用 3-Tesla 心脏磁共振成像量化全局心肌血流和心内膜下:心外膜灌注比;诱导性缺血定义为充血性心内膜下:心外膜灌注比<1.0。如果冠状动脉血流储备<2.5,则将患者分类为 MVD,如果冠状动脉血流储备≥2.5,则将患者分类为对照,研究人员对分类结果不知情。
共纳入 85 例患者(78%为女性,57±10 岁),其中 45 例(53%)被归类为 MVD。在 MVD 组中,82%的患者存在可诱导性缺血,而对照组为 22%(<0.001);全局心肌灌注储备为 2.01±0.41 和 2.68±0.49(<0.001)。在对照组中,冠状动脉灌注效率从休息时增加到运动时,在充血时没有变化(59±11%比 65±14%比 57±18%;=0.02 和=0.14)。相比之下,在 MVD 患者中,在两种应激形式下,灌注效率均下降(61±12 比 44±10 比 42±11%;均<0.001)。在冠状动脉血流储备<2.5 的患者中,62%存在功能性 MVD,最小 MR 正常(充血性 MR<2.5 mmHg/cm/s),38%存在结构性 MVD,充血性 MR 升高。与结构性 MVD 或对照组相比,功能性 MVD 患者的静息 MR 较低(4.2±1.0 mmHg/cm/s)(均<0.001)。在运动期间,结构性组的收缩压(188±25 mmHg)高于功能性 MVD 组(161±27 mmHg;=0.004)和对照组(156±30 mmHg;<0.001)。功能性和结构性 MVD 的应激性心肌灌注和运动性灌注效率值相似。
在患有心绞痛和非阻塞性冠状动脉疾病的患者中,冠状动脉血流储备的降低可识别出一组存在可诱导性缺血和运动时适应性生理反应受损的患者。我们已经确定了 MVD 的 2 种终末类型,它们对运动的全身血管反应不同;终末类型是否具有不同的预后或需要不同的治疗方法值得进一步研究。