Department of Health Services Research and Policy, London School of Hygiene and Tropical Medicine, London, UK
Department of Global Health and Development, London School of Hygiene and Tropical Medicine, London, UK.
BMJ Glob Health. 2020 May;5(5). doi: 10.1136/bmjgh-2019-002138.
Over the last 10 years, there has been a huge shift in malaria diagnosis in public health facilities, due to widespread deployment of rapid diagnostic tests (RDTs), which are accurate, quick and easy to use and inexpensive. There are calls for RDTs to be made available at-scale in the private retail sector where many people with suspected malaria seek care. Retail sector RDT use in sub-Saharan Africa (SSA) is limited to small-scale studies, and robust evidence on value-for-money is not yet available. We modelled the cost-effectiveness of introducing subsidised RDTs and supporting interventions in the SSA retail sector, in a context of a subsidy programme for first-line antimalarials.
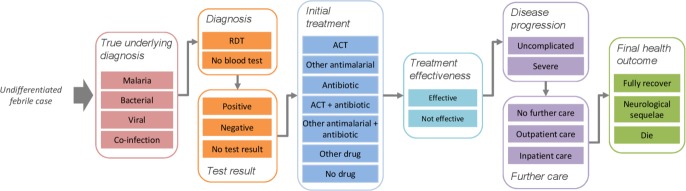
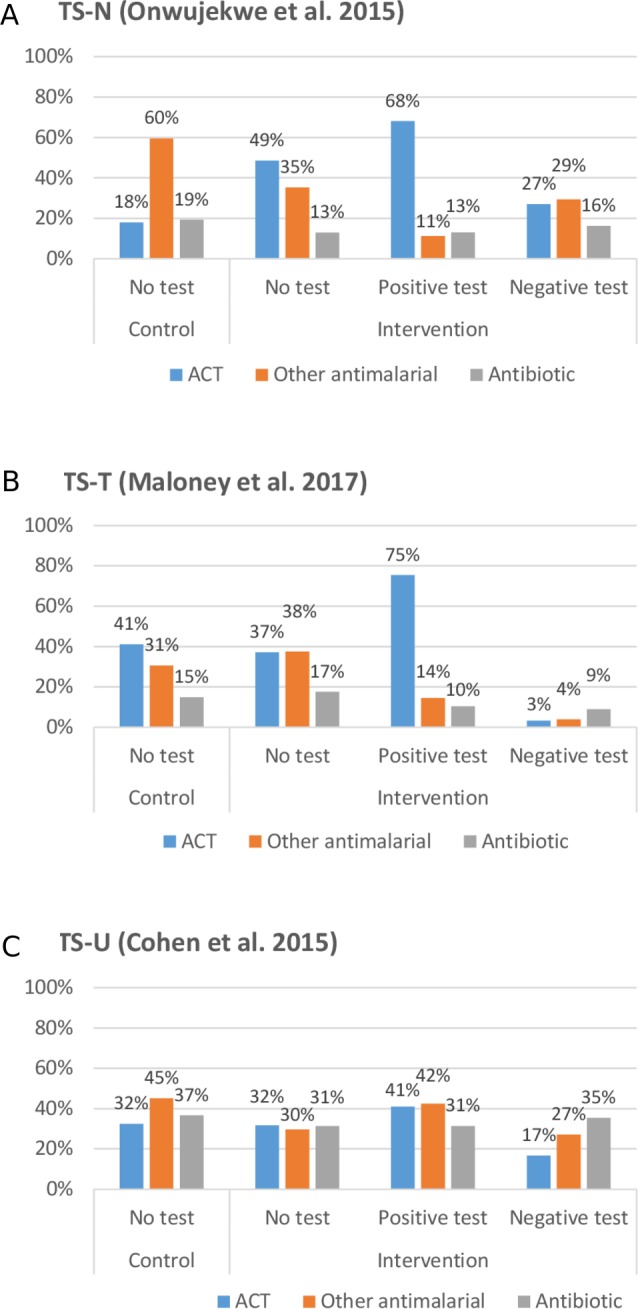
We developed a decision tree following febrile patients through presentation, diagnosis, treatment, disease progression and further care, to final health outcomes. We modelled results for three 'treatment scenarios', based on parameters from three small-scale studies in Nigeria (TS-N), Tanzania (TS-T) and Uganda (TS-U), under low and medium/high transmission (5% and 50% (parasite) positivity rates (PfPR), respectively).
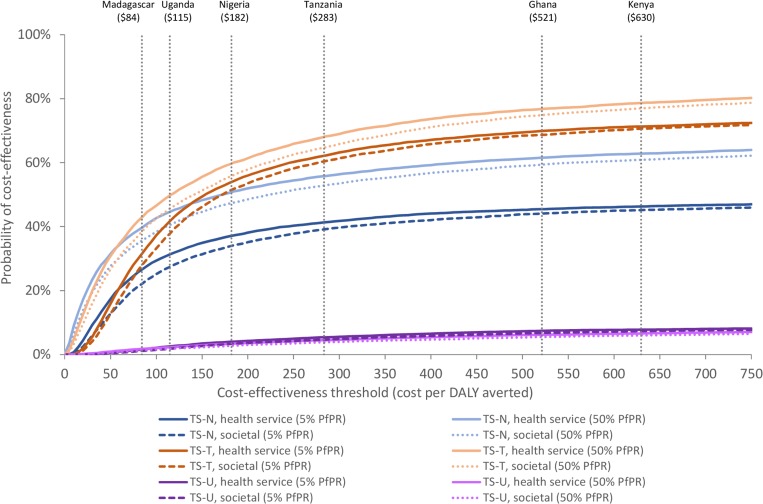
Cost-effectiveness varied considerably between treatment scenarios. Cost per disability-adjusted life year averted at 5% PfPR was US$482 (TS-N) and US$115 (TS-T) and at 50% PfPR US$44 (TS-N) and US$45 (TS-T), from a health service perspective. TS-U was dominated in both transmission settings.
The cost-effectiveness of subsidised RDTs is strongly influenced by treatment practices, for which further evidence is required from larger-scale operational settings. However, subsidised RDTs could promote increased use of first-line antimalarials in patients with malaria. RDTs may, therefore, be more cost-effective in higher transmission settings, where a greater proportion of patients have malaria and benefit from increased antimalarial use. This is contrary to previous public sector models, where RDTs were most cost-effective in lower transmission settings as they reduced unnecessary antimalarial use in patients without malaria.
在过去的 10 年中,由于快速诊断检测(RDT)的广泛应用,公共卫生机构中的疟疾诊断发生了巨大转变。RDT 准确、快速、易于使用且价格低廉。有人呼吁在私营零售部门大规模提供 RDT,因为许多疑似疟疾的人都在那里寻求治疗。撒哈拉以南非洲(SSA)的零售部门 RDT 使用仅限于小规模研究,并且尚未提供有关物有所值的可靠证据。我们模拟了在 SSA 零售部门引入补贴 RDT 和支持干预措施的成本效益,背景是为一线抗疟药物制定补贴计划。
我们根据来自尼日利亚(TS-N)、坦桑尼亚(TS-T)和乌干达(TS-U)的三项小规模研究的参数,通过提出、诊断、治疗、疾病进展和进一步护理,为三种“治疗方案”构建了决策树,最终达到健康结果。我们在低和中/高传播(分别为 5%和 50%的寄生虫阳性率(PfPR))下,为三种治疗方案构建了模型。
不同治疗方案的成本效益差异很大。在 PfPR 为 5%的情况下,从卫生服务角度来看,每避免一个残疾调整生命年的成本为 482 美元(TS-N)和 115 美元(TS-T),而在 PfPR 为 50%的情况下,每避免一个残疾调整生命年的成本为 44 美元(TS-N)和 45 美元(TS-T)。在两种传播环境下,TS-U 都处于劣势。
补贴 RDT 的成本效益受到治疗实践的强烈影响,因此需要从更大规模的运营环境中获得更多证据。然而,补贴 RDT 可以促进更多疟疾患者使用一线抗疟药物。因此,在传播率较高的地区,RDT 可能更具成本效益,因为更多的患者患有疟疾,并且受益于增加抗疟药物的使用。这与之前的公共部门模型相反,在低传播地区,RDT 最具成本效益,因为它们减少了没有疟疾的患者不必要的抗疟药物使用。