Department of Anesthesiology, Affiliated Hospital of Nanjing University of Chinese Medicine, Nanjing, Jiangsu, China (mainland).
Department of Acupuncture and Rehabilitation, Affiliated Hospital of Nanjing University of Chinese Medicine, Nanjing, Jiangsu, China (mainland).
Med Sci Monit. 2020 May 23;26:e920648. doi: 10.12659/MSM.920648.
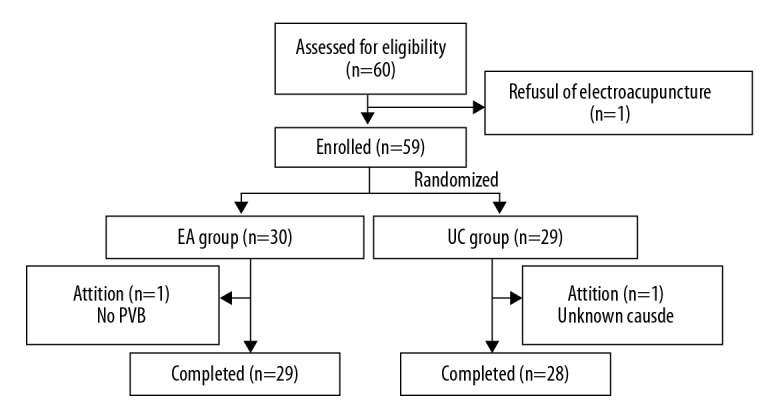
BACKGROUND The aim of this study was to study the feasibility and acceptability of electroacupuncture (EA) for preventing postoperative gastrointestinal complications in patients undergoing thoracoscopic segmentectomy/lobectomy. MATERIAL AND METHODS Sixty patients who underwent video-assisted thoracoscopic (VATS) segmentectomy/lobectomy received either EA treatments plus usual care (EA group) or usual care alone (UC group). Patients in the EA group were given 30 minutes of bilateral electroacupuncture on 3 acupoints [Neiguan (PC6), Zusanli (ST36), and Shangjuxu (ST37)] at 3 time points (24 hours before surgery, and 4 hours and 24 hours after surgery). The primary outcomes were recruitment, retention, acceptability of the EA intervention, incidence and severity of abdominal distension (AD), and time to first flatus and defecation. Secondary outcomes included postoperative nausea and vomiting (PONV), pain intensity, and duration of hospital stay. RESULTS We recruited 60 participants and 59 were randomized into 2 groups for this study: 30 in the EA group and 29 in the UC group. In total, 57 participants completed the study. With the exception of one participant in the EA group, all participants completed all three sessions of EA. The one exclusion was a case where a paravertebral block was not used during the surgery. Qualitative findings from the acceptability questionnaire indicated that participants viewed the EA treatment as acceptable. After EA treatment, there was a small but statistically significant improvement in participants' acceptance of EA for alleviating postoperative gastrointestinal discomfort (P=0.001). The EA group showed improved outcomes compared to the UC group in terms of time to first flatus (20.8±4.6 versus 24.1±6.2 hours, P=0.026) and defecation (53.9±6.0 versus 57.5±7.2 hours, P=0.046). No significant differences appeared regarding AD, rescue medication, or duration of hospitalization. PONV and pain intensity were similar in both groups at the recorded time periods. CONCLUSIONS EA is feasible and acceptable to patients undergoing VATS surgery. Our preliminary findings of EA promoting postoperative recovery of gastrointestinal function warrants large randomized controlled trials.
本研究旨在探讨电针对预防胸腔镜肺段切除术/肺叶切除术患者术后胃肠并发症的可行性和可接受性。
60 例行电视辅助胸腔镜(VATS)肺段切除术/肺叶切除术的患者接受电针治疗加常规护理(EA 组)或单纯常规护理(UC 组)。EA 组患者在术前 24 小时、术后 4 小时和 24 小时接受双侧电针刺激 3 个穴位[内关(PC6)、足三里(ST36)和上巨虚(ST37)],每次 30 分钟。主要结局指标为招募、保留、EA 干预的可接受性、腹胀(AD)的发生率和严重程度,以及首次排气和排便的时间。次要结局指标包括术后恶心和呕吐(PONV)、疼痛强度和住院时间。
共招募 60 名参与者,其中 59 名被随机分为 2 组进行本研究:EA 组 30 名,UC 组 29 名。共有 57 名参与者完成了研究。除了 EA 组的 1 名参与者外,所有参与者均完成了全部 3 次电针治疗。1 名排除病例是由于手术中未使用椎旁阻滞。可接受性问卷调查的定性结果表明,参与者认为电针治疗可以接受。电针治疗后,参与者对电针缓解术后胃肠不适的接受程度有了微小但具有统计学意义的改善(P=0.001)。与 UC 组相比,EA 组在首次排气(20.8±4.6 与 24.1±6.2 小时,P=0.026)和排便(53.9±6.0 与 57.5±7.2 小时,P=0.046)时间方面有改善。AD、解救药物和住院时间无显著差异。记录时间内,两组 PONV 和疼痛强度相似。
电针对于行 VATS 手术的患者是可行且可接受的。我们的初步发现表明,电针可促进胃肠功能的术后恢复,值得进行大规模随机对照试验。