Mayadev Jyoti, Nunes Ana T, Li Mary, Marcovitz Michelle, Lanasa Mark C, Monk Bradley J
GYN Cancers, Rebecca and John Moores Cancer Center, La Jolla, California, USA.
AstraZeneca R&D Gaithersburg, Gaithersburg, Maryland, USA.
Int J Gynecol Cancer. 2020 Jul;30(7):1065-1070. doi: 10.1136/ijgc-2019-001135. Epub 2020 May 23.
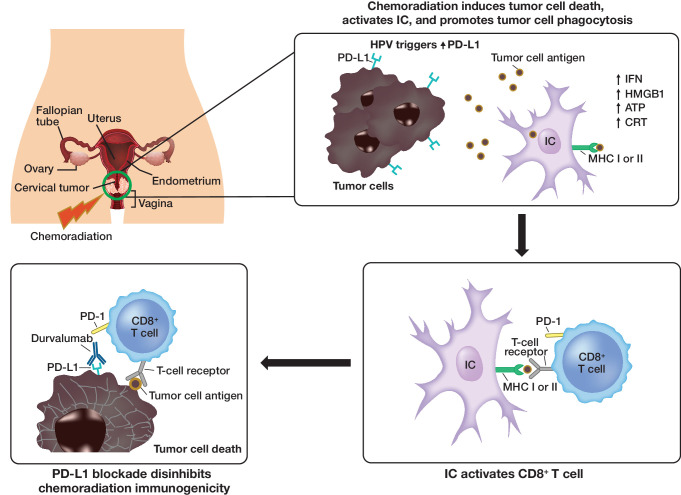
BackgroundConcurrent chemoradiotherapy is the standard of care for locally advanced cervical cancer. Concurrent chemoradiotherapy with programmed blockade of the cell death-1/programmed cell death-ligand 1 pathway may promote a more immunogenic environment through increased phagocytosis, cell death, and antigen presentation, leading to enhanced immune-mediated tumor surveillance.
The CALLA trial is designed to determine the efficacy and safety of the programmed cell death-ligand 1 blocking antibody, durvalumab, with and following concurrent chemoradiotherapy versus concurrent chemoradiotherapy alone in women with locally advanced cervical cancer.
Durvalumab concurrent with and following concurrent chemoradiotherapy will improve progression-free survival in patients with International Federation of Gynecology and Obstetrics (FIGO) 2009 stage IB2 to IVA cervical cancer compared with concurrent chemoradiotherapy alone.
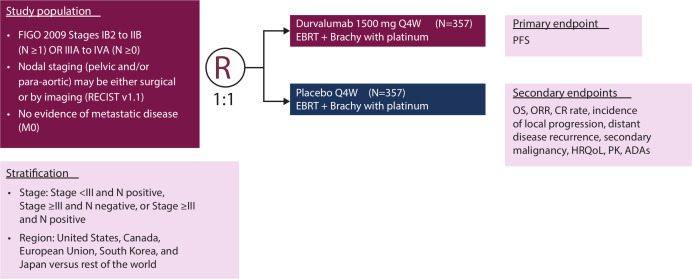
CALLA is a phase III, randomized, multicenter, international, double-blind, placebo-controlled study. Patients will be randomized 1:1 to receive either durvalumab (1500 mg intravenously (IV)) or placebo every 4 weeks for 24 cycles. All patients will receive external beam radiotherapy with cisplatin (40 mg/m) IV or carboplatin (area under the curve 2) IV once a week for 5 weeks, followed by image-guided brachytherapy.
MAJOR INCLUSION/EXCLUSION CRITERIA: The study will enroll immunotherapy-naïve adult patients with histologically confirmed cervical adenocarcinoma, cervical squamous, or adenosquamous carcinoma FIGO 2009 stages IB2-IIB node positive and stage IIIA-IVA with any node stage. Patients will have had no prior definitive surgical, radiation, or systemic therapy for cervical cancer.
The primary endpoint is progression-free survival (assessed by the investigator according to Response Evaluation Criteria in Solid Tumors v1.1, histopathological confirmation of local tumor progression or death).
Approximately 714 patients will be randomized 1:1 to receive either durvalumab + concurrent chemoradiotherapy or placebo + concurrent chemoradiotherapy.
Patient enrollment is continuing globally with an estimated completion date of April 2024.
NCT03830866.
背景
同步放化疗是局部晚期宫颈癌的标准治疗方法。同步放化疗联合程序性细胞死亡蛋白1/程序性细胞死亡配体1通路阻断可能通过增强吞噬作用、细胞死亡和抗原呈递促进更具免疫原性的环境,从而增强免疫介导的肿瘤监测。
CALLA试验旨在确定程序性细胞死亡配体1阻断抗体度伐利尤单抗在局部晚期宫颈癌女性患者中同步放化疗期间及之后使用与单独同步放化疗相比的疗效和安全性。
与单独同步放化疗相比,同步放化疗期间及之后使用度伐利尤单抗将改善国际妇产科联盟(FIGO)2009年IB2至IVA期宫颈癌患者的无进展生存期。
CALLA是一项III期、随机、多中心、国际、双盲、安慰剂对照研究。患者将按1:1随机分组,每4周接受一次度伐利尤单抗(1500毫克静脉注射)或安慰剂,共24个周期。所有患者将接受外照射放疗,同时静脉注射顺铂(40毫克/平方米)或卡铂(曲线下面积2),每周一次,共5周,随后进行图像引导下的近距离放疗。
主要纳入/排除标准:该研究将纳入未经免疫治疗的成年患者,组织学确诊为宫颈腺癌、宫颈鳞状癌或腺鳞癌,FIGO 2009年分期为IB2-IIB期淋巴结阳性以及任何淋巴结分期的IIIA-IVA期患者。患者既往未接受过针对宫颈癌的明确手术、放疗或全身治疗。
主要终点是无进展生存期(由研究者根据实体瘤疗效评价标准v1.1进行评估,通过组织病理学确认局部肿瘤进展或死亡)。
约714例患者将按1:1随机分组,接受度伐利尤单抗+同步放化疗或安慰剂+同步放化疗。
全球患者入组仍在继续,预计完成日期为2024年4月。
NCT03830866