Mayadev Jyoti, Zamarin Dmitriy, Deng Wei, Lankes Heather A, Pesci Giulio, Kim Hayeon, Chino Junzo P, Banbury Barbara, Sherry Ned, Sharon Elad, Ghamande Sharad A, Ferguson Catherine, Mell Loren, Holman Laura, Mathews Cara, O'Malley David, Olawaiye Alexander, Hopp Elizabeth, Leath Charles, Copeland Larry, Mannel Robert, O'Cearbhaill Roisin, Aghajanian Carol, Schilder Russell J
University of California San Diego, San Diego, USA.
Icahn School of Medicine at Mount Sinai, New York City, USA.
Nat Commun. 2025 Jan 9;16(1):553. doi: 10.1038/s41467-024-55200-2.
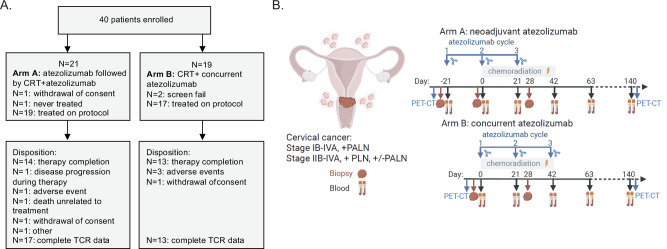
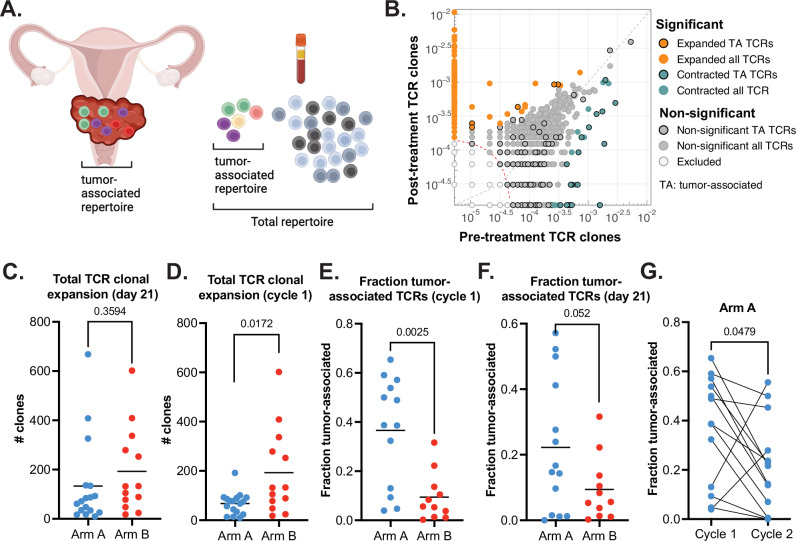
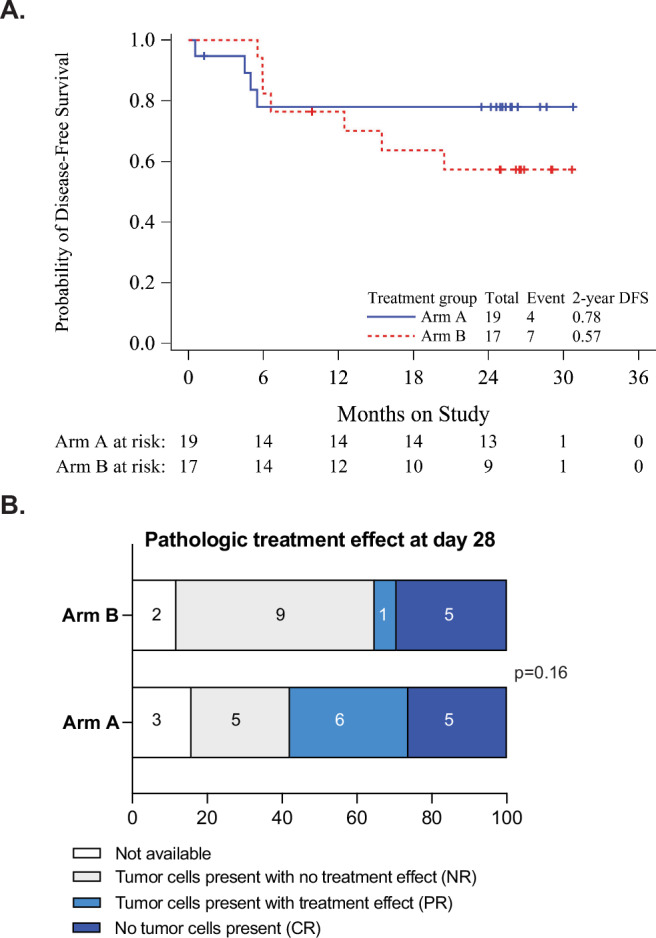
Combined immune checkpoint blockade (ICB) and chemoradiation (CRT) is approved in patients with locally advanced cervical cancer (LACC) but optimal sequencing of CRT and ICB is unknown. NRG-GY017 (NCT03738228) was a randomized phase I trial of atezolizumab (anti-PD-L1) neoadjuvant and concurrent with CRT (Arm A) vs. concurrent with CRT (Arm B) in patients with high-risk node-positive LACC. The primary endpoint was the fraction of expanded tumor-associated T-cell receptor (TCR) clones in blood at day 21 as a surrogate measure of anti-tumor immune response. Secondary objectives were safety and feasibility, 2-year disease-free survival (DFS), and predictive value of PD-L1 expression. Forty patients were randomized, 36 received treatment, and 25 were evaluable for the primary endpoint. After cycle 1, there was peripheral expansion of higher proportion of tumor-associated TCR clones in Arm A than in Arm B (p = 0.0025) that remained higher at day 21, meeting the pre-specified endpoint on two-sample T-test (p = 0.052), but not on sensitivity analysis by Wilcoxon test (p = 0.13). At the median follow up of 25.8 months, 2-year DFS was 76% in Arm A and 56% in Arm B (p = 0.28). There were no new safety signals. In conclusion, neoadjuvant ICB prior to CRT was safe and was associated with immunologically and clinically favorable outcomes, warranting larger confirmatory studies.
联合免疫检查点阻断(ICB)与放化疗(CRT)已被批准用于局部晚期宫颈癌(LACC)患者,但CRT和ICB的最佳序贯方案尚不清楚。NRG-GY017(NCT03738228)是一项I期随机试验,在高危淋巴结阳性LACC患者中比较阿特珠单抗(抗PD-L1)新辅助治疗并与CRT同期进行(A组)与仅与CRT同期进行(B组)的疗效。主要终点是第21天时血液中扩增的肿瘤相关T细胞受体(TCR)克隆比例,作为抗肿瘤免疫反应的替代指标。次要目标包括安全性和可行性、2年无病生存率(DFS)以及PD-L1表达的预测价值。40例患者被随机分组,36例接受了治疗,25例可用于评估主要终点。第1周期后,A组肿瘤相关TCR克隆在外周的扩增比例高于B组(p = 0.0025),在第21天时仍较高,在两样本t检验中达到预先设定的终点(p = 0.052),但在Wilcoxon检验的敏感性分析中未达到(p = 0.13)。在中位随访25.8个月时,A组2年DFS为76%,B组为56%(p = 0.28)。未发现新的安全信号。总之,CRT前进行新辅助ICB是安全的,并且与免疫和临床方面的良好结果相关,值得进行更大规模的验证性研究。