Malbrain Manu L N G, Langer Thomas, Annane Djillali, Gattinoni Luciano, Elbers Paul, Hahn Robert G, De Laet Inneke, Minini Andrea, Wong Adrian, Ince Can, Muckart David, Mythen Monty, Caironi Pietro, Van Regenmortel Niels
Department of Intensive Care Medicine, University Hospital Brussels (UZB), Laarbeeklaan 101, 1090, Jette, Belgium.
Faculty of Medicine and Pharmacy, Vrije Universiteit Brussel (VUB), Laarbeeklaan 103, Jette, 1090, Belgium.
Ann Intensive Care. 2020 May 24;10(1):64. doi: 10.1186/s13613-020-00679-3.
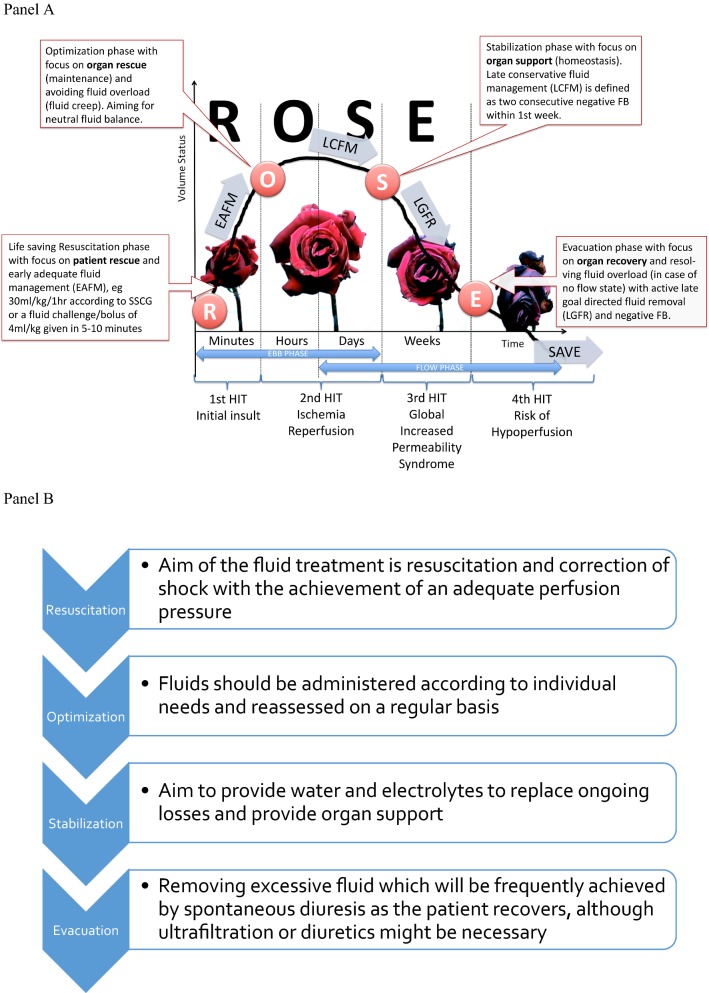
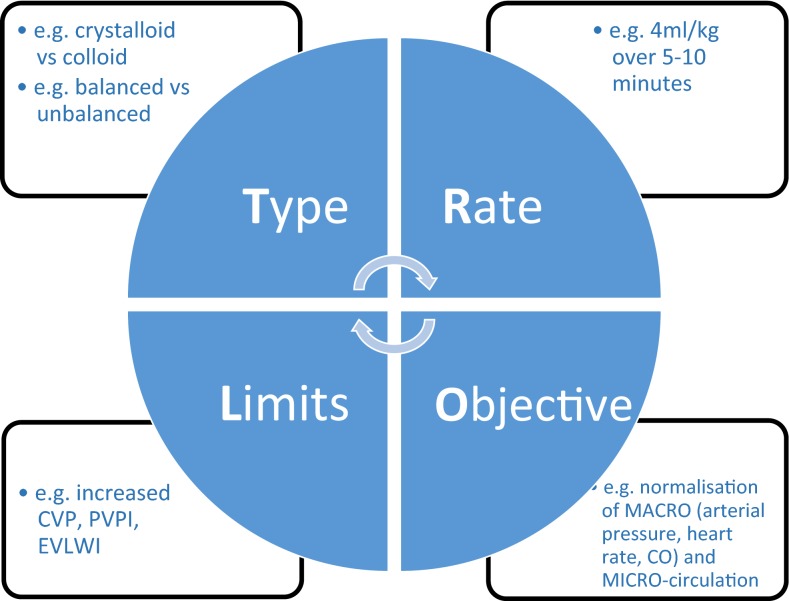
Intravenous fluid administration should be considered as any other pharmacological prescription. There are three main indications: resuscitation, replacement, and maintenance. Moreover, the impact of fluid administration as drug diluent or to preserve catheter patency, i.e., fluid creep, should also be considered. As for antibiotics, intravenous fluid administration should follow the four Ds: drug, dosing, duration, de-escalation. Among crystalloids, balanced solutions limit acid-base alterations and chloride load and should be preferred, as this likely prevents renal dysfunction. Among colloids, albumin, the only available natural colloid, may have beneficial effects. The last decade has seen growing interest in the potential harms related to fluid overloading. In the perioperative setting, appropriate fluid management that maintains adequate organ perfusion while limiting fluid administration should represent the standard of care. Protocols including a restrictive continuous fluid administration alongside bolus administration to achieve hemodynamic targets have been proposed. A similar approach should be considered also for critically ill patients, in whom increased endothelial permeability makes this strategy more relevant. Active de-escalation protocols may be necessary in a later phase. The R.O.S.E. conceptual model (Resuscitation, Optimization, Stabilization, Evacuation) summarizes accurately a dynamic approach to fluid therapy, maximizing benefits and minimizing harms. Even in specific categories of critically ill patients, i.e., with trauma or burns, fluid therapy should be carefully applied, considering the importance of their specific aims; maintaining peripheral oxygen delivery, while avoiding the consequences of fluid overload.
静脉输液应被视为与其他任何药物处方一样。主要有三个适应证:复苏、补充和维持。此外,还应考虑将输液用作药物稀释剂或保持导管通畅(即液体渗漏)的影响。对于抗生素而言,静脉输液应遵循四个“D”原则:药物、剂量、疗程、降阶梯。在晶体液中,平衡溶液可减少酸碱改变和氯化物负荷,应优先选用,因为这可能预防肾功能障碍。在胶体液中,白蛋白作为唯一可用的天然胶体,可能具有有益作用。在过去十年中,人们对与液体超负荷相关的潜在危害的关注度日益增加。在围手术期,适当的液体管理应在维持足够的器官灌注的同时限制液体输注,这应成为护理标准。已经提出了包括限制性持续输液并联合推注给药以实现血流动力学目标的方案。对于危重症患者也应考虑采用类似方法,这类患者内皮通透性增加使得该策略更为重要。在后期阶段可能需要积极的降阶梯方案。R.O.S.E.概念模型(复苏、优化、稳定、撤离)准确地总结了一种动态的液体治疗方法,可使益处最大化,危害最小化。即使在特定类别的危重症患者中,即创伤或烧伤患者,也应谨慎应用液体治疗,要考虑到其特定目标的重要性;维持外周氧输送,同时避免液体超负荷的后果。