Department of Surgery, Institut Jules Bordet, Université Libre de Bruxelles, 121, Boulevard de Waterloo, 1000, Brussels, Belgium.
Centre de Chirurgie Hépato-Biliaire de l'ULB (CCHB-ULB), Brussels, Belgium.
World J Surg Oncol. 2020 May 25;18(1):106. doi: 10.1186/s12957-020-01883-y.
The benefit of surgery in patients with non-colorectal non-neuroendocrine liver metastases (NCRNNELM) remains controversial. At the population level, several statistical prognostic factors and scores have been proposed but inconsistently verified. At the patient level, no selection criteria have been demonstrated to guide individual therapeutic decision making. We aimed to evaluate potential individual selection criteria to predict the benefit of surgery in patients undergoing treatment for NCRNNELM.
Data for 114 patients undergoing surgery for NCRNNELM were reviewed. In this population, we identified an early relapse group (ER), defined as patients with unresectable recurrence < 1 year postoperatively who did not benefit from surgery (N = 28), and a long-term survival group (LTS), defined as patients who were recurrence-free ≥ 5 years postoperatively and benefited from surgery (N = 20). Clinicopathologic parameters, the Association Française de Chirurgie (AFC) score, and a modified 4-point Clinical Risk Score (mCRS) (excluding CEA level) were analyzed and compared between LTS and ER groups.
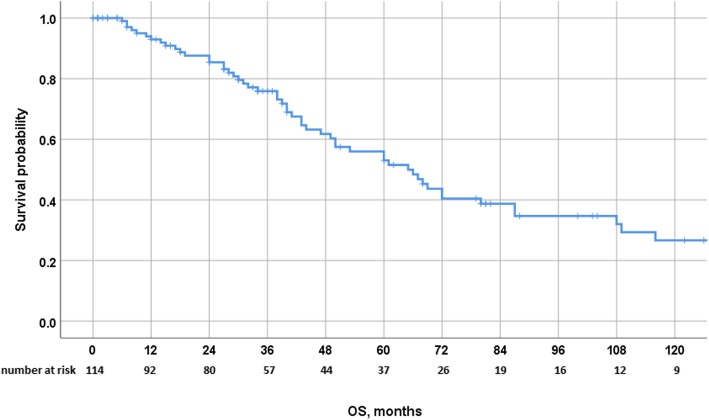
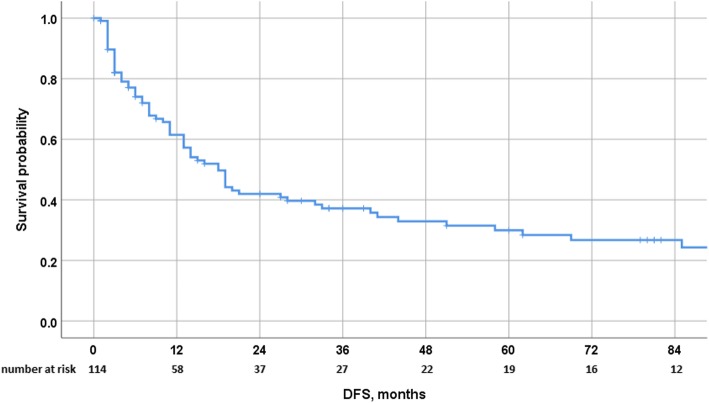
The majority of patients were female and a majority had an ASA score ≤ 2 at the time of liver surgery. The median age was 55 years. Almost half of the patients (46%) presented with a single-liver metastasis. Intermediate- and low-risk AFC scores represented 40% and 60% of the population, respectively. Five- and 10-year overall survival (OS) and disease-free survival (DFS) rates were 56% and 27%, and 30% and 12%, respectively. Negative prognostic factors were the size of liver metastases > 50 mm and delay between primary and NCRNNELM <24 months for OS and DFS, respectively. AFC score was not prognostic while high-risk mCRS (scores 3-4) was predictive for the poorer OS. The clinicopathologic parameters were similar in the ER and LTS groups, except the presence of N+ primary tumor, and the size of liver metastases was significantly higher in the ER group.
In patients with resectable NCRNNELM, no predictive factors or scores were found to accurately preoperatively differentiate individual cases in whom surgery would be futile from those in whom surgery could be associated with a significant oncological benefit.
手术治疗非结直肠神经内分泌肝脏转移瘤(NCRNNELM)患者的获益仍存在争议。在人群水平上,已经提出了几种统计预后因素和评分,但尚未得到一致验证。在个体水平上,尚无选择标准可指导个体治疗决策。本研究旨在评估潜在的个体选择标准,以预测接受 NCRNNELM 治疗的患者手术获益。
回顾了 114 例接受手术治疗的 NCRNNELM 患者的数据。在该人群中,我们确定了早期复发组(ER),定义为术后 1 年内无法切除的复发病例且手术无益的患者(n=28),以及长期生存组(LTS),定义为术后 5 年无复发且手术获益的患者(n=20)。比较了 LTS 组和 ER 组之间的临床病理参数、法国外科协会(AFC)评分和改良的 4 分临床风险评分(mCRS)(不包括 CEA 水平)。
大多数患者为女性,且多数患者在肝切除术时的美国麻醉医师协会(ASA)评分为≤2。中位年龄为 55 岁。近一半的患者(46%)为单发肝转移。中危和低危 AFC 评分分别占人群的 40%和 60%。5 年和 10 年总生存(OS)和无病生存(DFS)率分别为 56%和 27%,30%和 12%。OS 和 DFS 的负预后因素分别为肝转移灶直径>50mm 和原发肿瘤与 NCRNNELM 之间的时间间隔<24 个月。AFC 评分无预后意义,而高危 mCRS(评分 3-4)与较差的 OS 相关。ER 组和 LTS 组的临床病理参数相似,除了存在 N+原发肿瘤外,ER 组的肝转移灶直径明显更大。
在可切除的 NCRNNELM 患者中,尚未发现预测因素或评分能够在术前准确区分手术无益和可获得显著肿瘤获益的个体病例。