W Kim Daniel, Raoof Sana, Lamba Nayan, Lee Grace, S Bitterman Danielle, R Mahal Amandeep, N Sanford Nina, B Lam Miranda, J Mamon Harvey
Department of Radiation Oncology, Dana-Farber Cancer Institute/Brigham and Women's Hospital, Boston, MA 02115, USA.
Harvard Medical School, Boston, MA 02115, USA.
Mol Clin Oncol. 2020 Jul;13(1):27-32. doi: 10.3892/mco.2020.2044. Epub 2020 May 11.
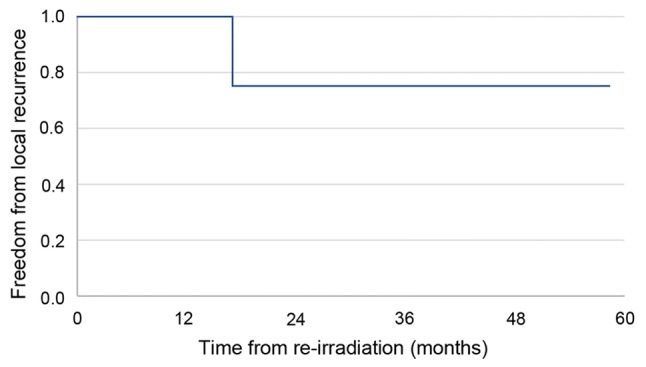
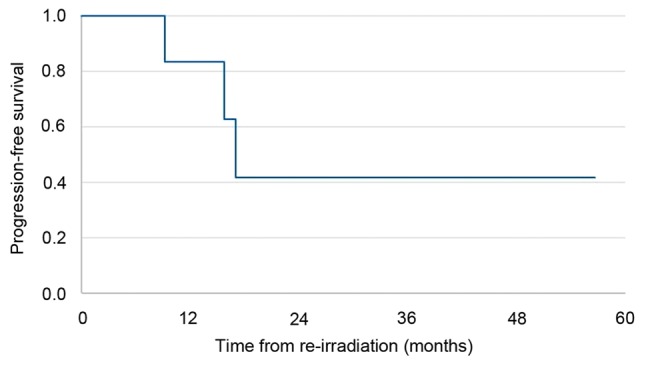
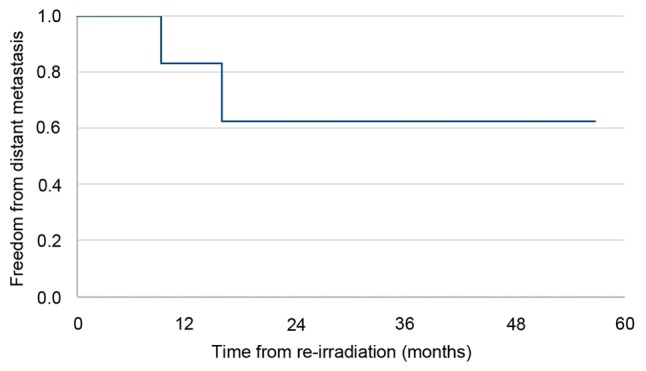
There are few treatment guidelines for locally recurrent esophageal cancer after trimodality treatment (pre-operative chemoradiation followed by surgery) in patients with a poor performance status. The purpose of this single institutional, retrospective study was to evaluate the clinical outcomes and toxicities of definitive-intent re-irradiation for patients with recurrent esophageal cancer with a poor performance status [ECOG (Eastern Cooperative Oncology Group) ≥2]. Seven patients were identified with a median age of 74 years (range, 61-81 years). Four patients were ECOG 2 and three patients were ECOG 3. The median follow-up time after re-irradiation was 49 months. The median interval between initial radiotherapy and re-treatment was 32 months. Six patients received concurrent chemotherapy [carboplatin + paclitaxel in three patients; folinic acid, fluorouracil, oxaliplatin (FOLFOX) + 5-fluorouracil in one patient; FOLFOX in one patient, and capecitabine in one patient]. At the last follow-up, the six patients who underwent concurrent chemotherapy had stable disease (86%), while the one who did not receive chemotherapy progressed (14%). Two patients developed metastases. Three patients developed acute (<6 months) grade 4 toxicities (dysphagia, anemia, esophagitis). There were no early deaths attributable to treatment. Late toxicities (>6 months) were limited to grades 1 and 2 dysphagia and pneumonitis in four patients. In conclusion, definitive re-irradiation of recurrent esophageal cancer in patients with a poor performance status appears to be safe with acceptable acute toxicity and late complications. It also appears to result in durable local control when combined with chemotherapy, albeit with a small number of patients and limited follow-up.
对于身体状况较差的患者,在接受三联疗法(术前放化疗后手术)后出现局部复发性食管癌,几乎没有治疗指南。这项单机构回顾性研究的目的是评估对身体状况较差[东部肿瘤协作组(ECOG)≥2]的复发性食管癌患者进行根治性再照射的临床疗效和毒性。确定了7例患者,中位年龄为74岁(范围61 - 81岁)。4例患者ECOG评分为2分,3例患者ECOG评分为3分。再照射后的中位随访时间为49个月。初始放疗与再治疗之间的中位间隔时间为32个月。6例患者接受了同步化疗[3例患者使用卡铂 + 紫杉醇;1例患者使用亚叶酸、氟尿嘧啶、奥沙利铂(FOLFOX) + 5 - 氟尿嘧啶;1例患者使用FOLFOX,1例患者使用卡培他滨]。在最后一次随访时,接受同步化疗的6例患者病情稳定(86%),而未接受化疗的1例患者病情进展(14%)。2例患者发生转移。3例患者出现急性(<6个月)4级毒性反应(吞咽困难、贫血、食管炎)。没有因治疗导致的早期死亡。晚期毒性反应(>6个月)仅限于4例患者出现1级和2级吞咽困难及肺炎。总之,对身体状况较差的复发性食管癌患者进行根治性再照射似乎是安全的,急性毒性和晚期并发症均可接受。与化疗联合使用时,似乎也能实现持久的局部控制,尽管患者数量较少且随访有限。