Lagziel Tomer, Quiroga Luis, Ramos Margarita, Hultman Charles S, Asif Mohammed
Plastic Surgery, Johns Hopkins University School of Medicine, Baltimore, USA.
Medicine, Tel-Aviv University, Sackler School of Medicine, Tel-Aviv, ISR.
Cureus. 2020 May 19;12(5):e8198. doi: 10.7759/cureus.8198.
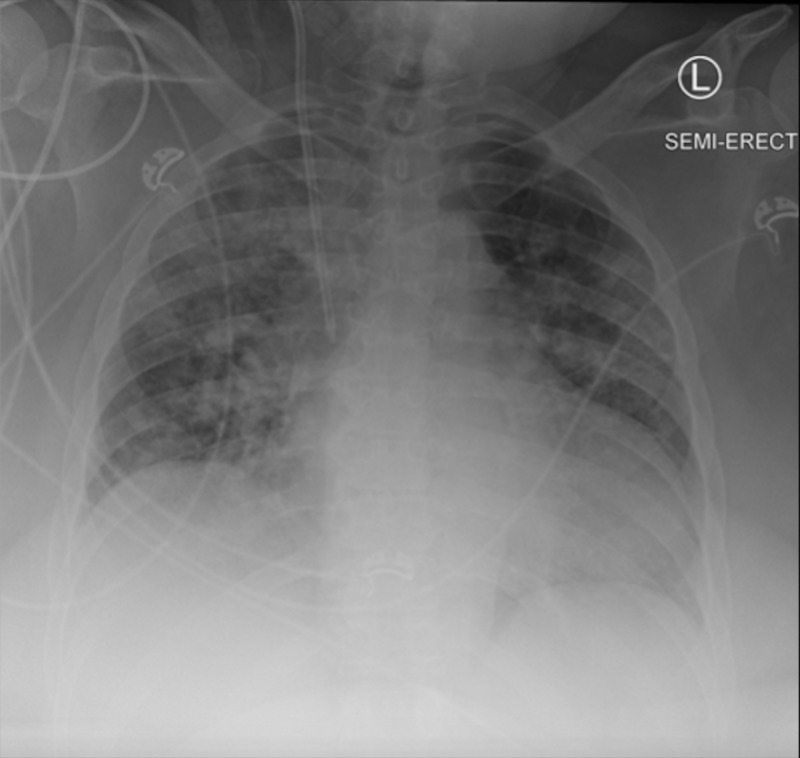
The recent outbreak of COVID-19 has put significant strain on the current health system and has exposed dangers previously overlooked. The pathogen known as severe acute respiratory syndrome coronavirus 2 (SARS-COV-2), is notable for attacking the pulmonary system causing acute respiratory distress, but it can also severely affect other systems in at-risk individuals including cardiovascular compromise, gastrointestinal distress, acute kidney injury, coagulopathies, cutaneous manifestations, and ultimately death from multi-organ failure. Unfortunately, the reliability of negative test results is questionable and the high infectious burden of the virus calls for extended safety precautions, especially in symptomatic patients. We present a confirmed COVID-19 case that was transferred to our burn center for concern of Steven Johnson syndrome/toxic epidermal necrolysis (SJS/TEN) overlap syndrome after having two negative confirmatory COVID-19 tests at an outside hospital. A 58-year-old female with a history of morbid obesity, HTN, gout, CML managed with imatinib, and chronic kidney disease presented as a transfer from a community hospital to our burn center. The patient was admitted to her community hospital with febrile, acute respiratory distress. Imaging and clinical presentation was consistent with COVID-19 and lab tests for the pathogen were ordered. During observation, while waiting for results, she was placed under patient under investigation (PUI) protocol. Once negative results were obtained, the PUI protocol was abandoned despite ongoing symptoms. Subsequently, dermatological symptoms developed and transfer to our burn center was initiated. After a second negative test result, the symptomatic patient was transferred to our burn center for expert wound management. Given the lack of resolve of respiratory symptoms and concern for the burn patient population, the patient was placed in PUI protocol and an internal COVID-19 was ordered. The patient's initial exam under standard COVID-19 airborne precautions revealed 5% total body surface area of loss of epidermis affecting bilateral thighs, bilateral arms, and face. A dermatopathological biopsy suggested a bullous drug reaction with an erythema multiform-like reaction pattern versus SJS/TEN. Moreover, the internal COVID-19 test returned positive. The delayed positive test results and complicated hospital course with our patient required us to scale back and notify every patient and staff member whom they came in contact with, across multiple institutions. We suggest that whenever a suspected COVID-19 patient is transferred to a specialized center, they should be isolated and re-checked before joining the new patient population for treatment of the unique condition.
近期爆发的新型冠状病毒肺炎(COVID-19)给当前的医疗系统带来了巨大压力,也暴露了此前被忽视的危险。这种被称为严重急性呼吸综合征冠状病毒2(SARS-CoV-2)的病原体,以侵袭肺部系统导致急性呼吸窘迫而闻名,但它也会严重影响高危个体的其他系统,包括心血管功能受损、胃肠道不适、急性肾损伤、凝血功能障碍、皮肤表现,最终可导致多器官功能衰竭死亡。不幸的是,阴性检测结果的可靠性存疑,而且该病毒的高传染性要求采取更严格的安全预防措施,尤其是对有症状的患者。我们报告了一例确诊的COVID-19病例,该患者在外部医院进行了两次COVID-19确诊检测均为阴性后,因疑似史蒂文斯-约翰逊综合征/中毒性表皮坏死松解症(SJS/TEN)重叠综合征而被转至我们的烧伤中心。一名58岁女性,有肥胖症、高血压、痛风病史,慢性粒细胞白血病正在接受伊马替尼治疗,还有慢性肾病,从社区医院转至我们的烧伤中心。该患者因发热、急性呼吸窘迫入住社区医院。影像学检查和临床表现与COVID-19相符,并已安排对病原体进行实验室检测。在观察等待结果期间,她被按照待排查患者(PUI)方案进行管理。一旦获得阴性结果,尽管症状仍在持续,PUI方案也被终止。随后,出现了皮肤症状,并开始转至我们的烧伤中心。在第二次检测结果为阴性后,这名有症状的患者被转至我们的烧伤中心接受专业伤口处理。鉴于呼吸道症状未缓解且考虑到烧伤患者群体的情况,该患者被重新纳入PUI方案,并进行了一次内部COVID-19检测。在标准的COVID-19空气传播预防措施下对患者进行的初步检查发现,患者双侧大腿、双侧手臂和面部表皮缺失总面积达5%。皮肤病理活检提示为大疱性药物反应,呈多形红斑样反应模式,而非SJS/TEN。此外,内部COVID-19检测结果呈阳性。我们的患者检测结果延迟呈阳性以及复杂的住院过程,要求我们缩减规模并通知了多家机构中与该患者接触过的每一位患者和工作人员。我们建议,每当疑似COVID-19患者被转至专科中心时,在加入新的患者群体接受特殊疾病治疗之前,都应进行隔离并重新检查。