Department of General Practice and Emergency Medicine, Maharajgunj Medical Campus, Institute of Medicine, Tribhuvan University, Kathmandu, Nepal.
BMC Emerg Med. 2020 May 26;20(1):43. doi: 10.1186/s12873-020-00337-8.
Sepsis is a common problem encountered in the emergency room which needs to be intervened early. Predicting prognosis is always a difficult task in busy emergency rooms using present scores, which has several variables to calculate. Red cell distribution width (RDW) is an easy, cheap, and efficacious score to predict the severity and mortality of patients with sepsis.
This prospective analytical study was conducted in the emergency room of Tribhuvan University Teaching Hospital among the patients age ≥ 16 years and with a clinical diagnosis of sepsis using qSOFA score. 148 patients were analyzed in the study by using a non-probability purposive sampling method.
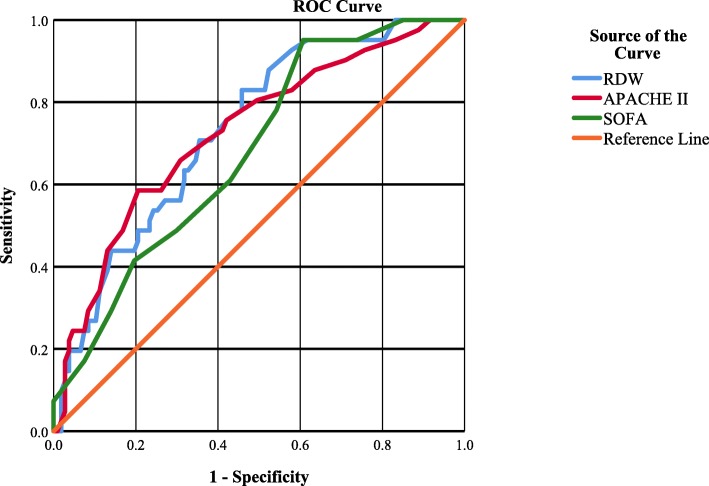
RDW has fair efficacy to predict the mortality in sepsis (Area under the Curve of 0.734; 95% C. I = 0.649-0.818; p-value = 0.000) as APACHE II (AUC of 0.728; 95% C. I = 0.637 to 0.819; p-value = 0.000) or SOFA (AUC of 0.680, 95% C. I = 0.591-0.770; p-value = 0.001). Youden Index was maximum (37%) at RDW value 14.75, which has a sensitivity of 83% (positive likelihood ratio = 1.81) and specificity of 54% (negative likelihood ratio = 0.32). Out of 44 patients with septic shock 16 died (36.4%) and among 104 patients without septic shock, 24 died (22.9%) which had the odds ratio of 0.713 (p = 0.555, 95% C. I = 0.231-2.194). Overall mortality was 27.02% (n = 40). RDW group analysis showed no mortality in RDW < 13.1 group, 3.6% mortality in 13.1 to 14 RDW group, 22.0% mortality in 14 to > 15.6 RDW group and 45.9% mortality in > 15.6 RDW group. Significant mortality difference was seen in 14 to > 15.6 and > 15.6 RDW subgroups with a p-value of 0.003 and 0.008 respectively.
Area under the curve value for RDW is fair enough to predict the mortality of patients with sepsis in the emergency room. It can be integrated with other severity scores (APACHE II or SOFA score) for better prediction of prognosis of septic patients.
脓毒症是急诊科常见的问题,需要及早干预。使用现有评分预测预后一直是繁忙急诊科的一项艰巨任务,因为这些评分有多个变量需要计算。红细胞分布宽度(RDW)是一种简单、廉价且有效的评分,可以预测脓毒症患者的严重程度和死亡率。
这项前瞻性分析性研究在特里布万大学教学医院的急诊科进行,纳入年龄≥16 岁且临床诊断为脓毒症的患者,使用 qSOFA 评分。研究采用非概率目的性抽样方法,共分析了 148 例患者。
RDW 对预测脓毒症患者的死亡率具有良好的效果(曲线下面积为 0.734;95%置信区间为 0.649-0.818;p 值=0.000),与急性生理与慢性健康状况评分 II(AUC 为 0.728;95%置信区间为 0.637-0.819;p 值=0.000)或序贯器官衰竭评估(SOFA)评分(AUC 为 0.680,95%置信区间为 0.591-0.770;p 值=0.001)相当。RDW 值为 14.75 时约登指数最大(37%),此时的灵敏度为 83%(阳性似然比=1.81),特异性为 54%(阴性似然比=0.32)。44 例脓毒性休克患者中有 16 例死亡(36.4%),104 例无脓毒性休克患者中有 24 例死亡(22.9%),其比值比为 0.713(p=0.555,95%置信区间为 0.231-2.194)。总的死亡率为 27.02%(n=40)。RDW 组分析显示,RDW<13.1 组无死亡,13.1≤RDW<14 组死亡率为 3.6%,14≤RDW<15.6 组死亡率为 22.0%,RDW>15.6 组死亡率为 45.9%。在 14≤RDW<15.6 和 RDW>15.6 亚组中,死亡率差异有统计学意义(p 值分别为 0.003 和 0.008)。
RDW 的曲线下面积足以预测急诊科脓毒症患者的死亡率。它可以与其他严重程度评分(急性生理与慢性健康状况评分 II 或 SOFA 评分)结合使用,以更好地预测脓毒症患者的预后。