Ju Xue-Feng, Wang Fei, Wang Li, Wu Xiao, Jiang Ting-Ting, You Da-Li, Yang Bing-Hua, Xia Jian-Jun, Hu Shan-You
Department of Emergency Medicine, Shanghai Jiading District Central Hospital, Shanghai 201800, China.
Department of Critical Care Medicine, Shanghai Jiading District Central Hospital, Shanghai 201800, China.
Chin Med J (Engl). 2017 May 20;130(10):1189-1195. doi: 10.4103/0366-6999.205858.
The normal range of red cell distribution width (RDW) level is <15%. Several studies have indicated that a high RDW level was associated with mortality in critically ill patients, and the patients with a high RDW level need increased focus in clinical practice. In view of the difficulty in defining the specific value of high RDW level, the key is to focus on the patient with the level beyond the normal upper limit. This study aimed to determine whether dynamic change of RDW levels, rather than the level itself, is predictive of death in elderly patients with septic shock when RDW level is beyond 15%.
Between September 2013 and September 2015, the elderly septic shock patients with RDW level beyond 15% were enrolled in this study. The RDW levels were measured at enrollment (day 1), and days 4 and 7 after enrollment. Sequential Organ Failure Assessment (SOFA) scores were recorded simultaneously.
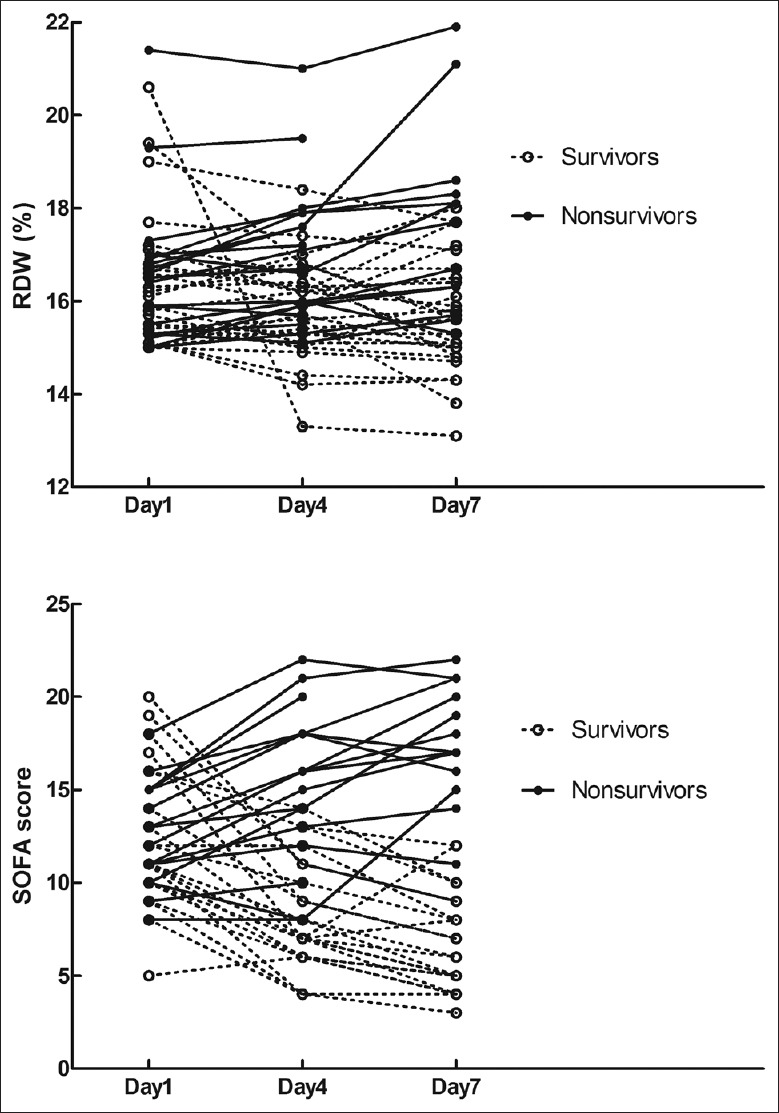
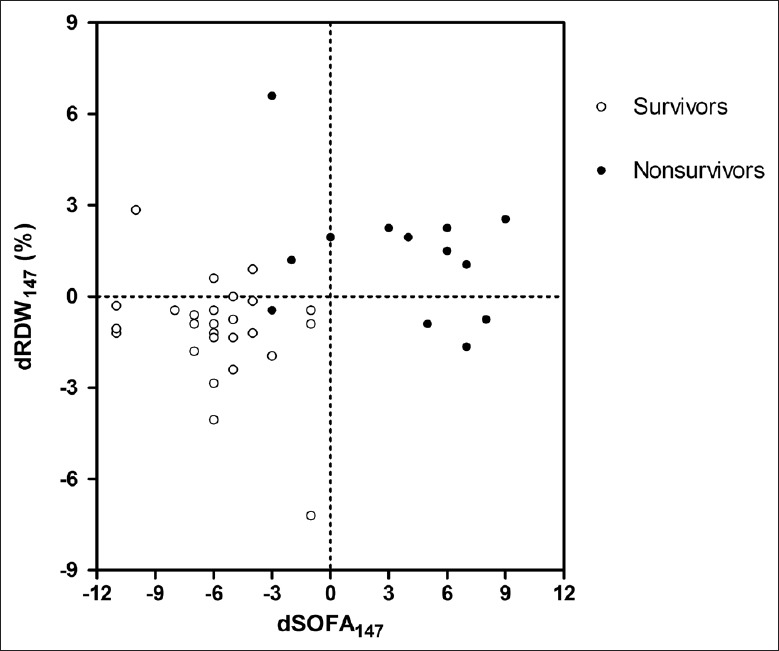
A total of 45 patients, including 32 males and 13 females, were included in the final analysis. Based on their hospital outcomes, these patients were divided into the survivor group (n = 26) and the nonsurvivor group (n = 19). There were no significant differences in age, gender, body mass index, initial level of RDW, Acute Physiology and Chronic Health Evaluation II scores, and SOFA scores between survivors and nonsurvivors. At days 4 and 7 measurement, both RDW level (median [interquartile range]: day 4: 15.8 [2.0]% vs. 16.7 [2.0]%, P= 0.011; and day 7: 15.6 [1.8]% vs. 17.7 [2.5]%, P= 0.001) and SOFA scores (day 4: 7.0 [4.0] vs. 16.0 [5.0], P< 0.001, day 7: 5.5 [4.0] vs. 17.0 [5.0], P< 0.001) were significantly lower in survivors than those in nonsurvivors. Dynamic changes of RDW and SOFA scores in survivor group were significantly different from those in nonsurvivor group (all P< 0.05). Continuous increase in RDW level was observed in 10 of the 13 nonsurvivors, but only in 3 of the 26 survivors. The level of RDW7 and dynamic changes significantly correlated with their counterparts of SOFA scores (all P< 0.05), whereas the levels of RDW1 and RDW4 had no significant correlation with their counterparts of SOFA scores (all P> 0.05).
Continuous increase in RDW level, rather than the level of RDW itself, was more useful in predicting hospital death in elderly patients with septic shock when the level of RDW was >15%. The dynamic changes of RDW were highly correlated with the SOFA score in the patients.
红细胞分布宽度(RDW)水平的正常范围<15%。多项研究表明,RDW水平升高与危重症患者的死亡率相关,临床实践中需要对RDW水平升高的患者给予更多关注。鉴于难以确定RDW高水平的具体数值,关键在于关注超出正常上限水平的患者。本研究旨在确定当RDW水平超过15%时,RDW水平的动态变化而非水平本身是否可预测老年感染性休克患者的死亡。
2013年9月至2015年9月,纳入RDW水平超过15%的老年感染性休克患者。在入组时(第1天)、入组后第4天和第7天测量RDW水平。同时记录序贯器官衰竭评估(SOFA)评分。
最终分析纳入45例患者,包括32例男性和13例女性。根据住院结局,这些患者分为存活组(n = 26)和非存活组(n = 19)。存活者和非存活者在年龄、性别、体重指数、RDW初始水平、急性生理与慢性健康状况评分II和SOFA评分方面无显著差异。在第4天和第7天测量时,存活者的RDW水平(中位数[四分位间距]:第4天:15.8[2.0]%对16.7[2.0]%,P = 0.011;第7天:15.6[1.8]%对17.7[2.5]%,P = 0.001)和SOFA评分(第4天:7.0[4.0]对16.0[5.0],P<0.001,第7天:5.5[4.0]对17.0[5.0],P<0.001)均显著低于非存活者。存活组RDW和SOFA评分的动态变化与非存活组显著不同(均P<0.05)。13例非存活者中有10例观察到RDW水平持续升高,而26例存活者中仅3例。RDW7水平和动态变化与SOFA评分的对应指标显著相关(均P<0.05),而RDW1和RDW4水平与SOFA评分对应指标无显著相关性(均P>0.05)。
当RDW水平>15%时,RDW水平的持续升高而非RDW本身的水平更有助于预测老年感染性休克患者的院内死亡。患者中RDW的动态变化与SOFA评分高度相关。