King's Health Economics, Institute of Psychiatry, Psychology, and Neuroscience, King's College London, London, United Kingdom.
Health Economics and Decision Science, University of Sheffield School of Health and Related Research, Sheffield, United Kingdom.
JAMA Netw Open. 2020 May 1;3(5):e205888. doi: 10.1001/jamanetworkopen.2020.5888.
The existing economic models for schizophrenia often have 3 limitations; namely, they do not cover nonpharmacologic interventions, they report inconsistent conclusions for antipsychotics, and they have poor methodologic quality.
To develop a whole-disease model for schizophrenia and use it to inform resource allocation decisions across the entire care pathway for schizophrenia in the UK.
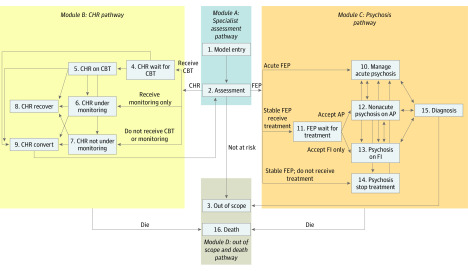
DESIGN, SETTING, AND PARTICIPANTS: This decision analytical model used a whole-disease model to simulate the entire disease and treatment pathway among a simulated cohort of 200 000 individuals at clinical high risk of psychoses or with a diagnosis of psychosis or schizophrenia being treated in primary, secondary, and tertiary care in the UK. Data were collected March 2016 to December 2018 and analyzed December 2018 to April 2019.
The whole-disease model used discrete event simulation; its structure and input data were informed by published literature and expert opinion. Analyses were conducted from the perspective of the National Health Service and Personal Social Services over a lifetime horizon. Key interventions assessed included cognitive behavioral therapy, antipsychotic medication, family intervention, inpatient care, and crisis resolution and home treatment team.
Life-time costs and quality-adjusted life-years.
In the simulated cohort of 200 000 individuals (mean [SD] age, 23.5 [5.1] years; 120 800 [60.4%] men), 66 400 (33.2%) were not at risk of psychosis, 69 800 (34.9%) were at clinical high risk of psychosis, and 63 800 (31.9%) had psychosis. The results of the whole-disease model suggest the following interventions are likely to be cost-effective at a willingness-to-pay threshold of £20 000 ($25 552) per quality-adjusted life-year: practice as usual plus cognitive behavioral therapy for individuals at clinical high risk of psychosis (probability vs practice as usual alone, 0.96); a mix of hospital admission and crisis resolution and home treatment team for individuals with acute psychosis (probability vs hospital admission alone, 0.99); amisulpride (probability vs all other antipsychotics, 0.39), risperidone (probability vs all other antipsychotics, 0.30), or olanzapine (probability vs all other antipsychotics, 0.17) combined with family intervention for individuals with first-episode psychosis (probability vs family intervention or medication alone, 0.58); and clozapine for individuals with treatment-resistant schizophrenia (probability vs other medications, 0.81).
The results of this study suggest that the current schizophrenia service configuration is not optimal. Cost savings and/or additional quality-adjusted life-years may be gained by replacing current interventions with more cost-effective interventions.
现有的精神分裂症经济模型通常存在 3 个局限性;即,它们不包括非药物干预措施,对于抗精神病药物的报告结论不一致,且方法学质量较差。
开发一种针对精神分裂症的全疾病模型,并在英国精神分裂症整个护理路径中使用该模型为资源分配决策提供信息。
设计、设置和参与者:该决策分析模型使用全疾病模型来模拟 200000 名处于精神病高危状态或正在初级、二级和三级护理中接受精神病或精神分裂症治疗的个体的整个疾病和治疗途径,这些个体来自于一个模拟队列。数据于 2016 年 3 月至 2018 年 12 月收集,并于 2018 年 12 月至 2019 年 4 月进行分析。
全疾病模型使用离散事件模拟;其结构和输入数据来自已发表的文献和专家意见。分析从国民保健服务和个人社会服务的角度在终生范围内进行。评估的关键干预措施包括认知行为疗法、抗精神病药物、家庭干预、住院治疗以及危机解决和家庭治疗小组。
终生成本和质量调整生命年。
在 200000 名个体的模拟队列中(平均[标准差]年龄,23.5[5.1]岁;120800[60.4%]为男性),66400(33.2%)没有精神病高危,69800(34.9%)处于精神病高危,63800(31.9%)患有精神病。全疾病模型的结果表明,在 20000 英镑(25552 美元)每质量调整生命年的意愿支付阈值下,以下干预措施可能具有成本效益:对精神病高危个体进行常规治疗加认知行为疗法(与常规治疗相比的可能性,0.96);对急性精神病个体采用混合住院和危机解决及家庭治疗小组(与住院治疗相比的可能性,0.99);氨磺必利(与所有其他抗精神病药物相比的可能性,0.39)、利培酮(与所有其他抗精神病药物相比的可能性,0.30)或奥氮平(与所有其他抗精神病药物相比的可能性,0.17)联合家庭干预用于治疗首发精神病个体(与家庭干预或药物治疗相比的可能性,0.58);氯氮平用于治疗难治性精神分裂症个体(与其他药物相比的可能性,0.81)。
这项研究的结果表明,目前的精神分裂症服务配置并不理想。通过用更具成本效益的干预措施替代当前的干预措施,可能会节省成本和/或增加质量调整生命年。