Pessia Beatrice, Romano Lucia, Giuliani Antonio, Lazzarin Gianni, Carlei Francesco, Schietroma Mario
Department of Surgery, Department of Applied Clinical Science and Biotechnology, University of L'Aquila, L'Aquila, Italy.
Ann Med Surg (Lond). 2020 May 12;55:36-46. doi: 10.1016/j.amsu.2020.04.016. eCollection 2020 Jul.
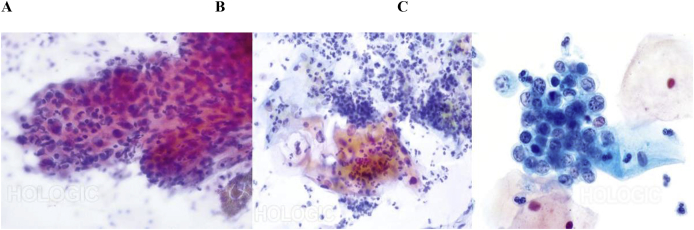
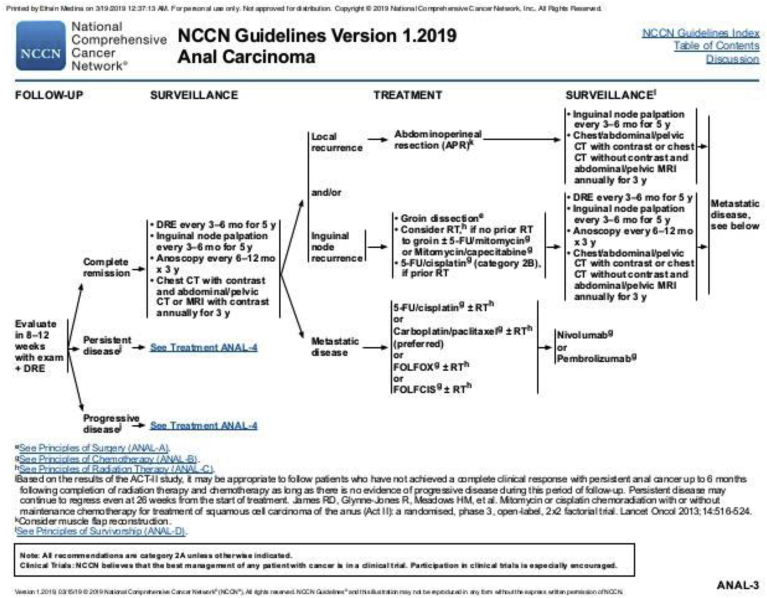
The incidence of anal cancer has increased during the second half of the 20th century, with an incidence rate over 2.9% greater than in the decade of 1992-2001. Yet, it still constitutes a small percentage, about 4%, of all anorectal tumours. Its risk factors are human papillomavirus infection, a history of sexually transmitted diseases, a history of vulvar or cervical carcinoma, immunosuppression related to human immunodeficiency virus infection or after organ transplantation, haematological or immunological disorders, and smoking. The most frequent symptom is rectal bleeding (45%), followed by anal pain, and sensation of a rectal mass. The diagnosis requires clinical examination, palpation of the inguinal lymph nodes, high resolution anoscopy followed by fine-needle aspiration biopsy or core biopsy. Subsequent histologic diagnosis is necessary, as well as computed tomography or magnetic resonance imaging evaluation of the pelvic lymph nodes. Since 1980, patients with a diagnosis of anal cancer have shown a significant improvement in survival. In Europe during the years 1983-1994, 1-year survival increased from 78% to 81%, and the improvement over 5 years was between 48% and 54%. Prior to 1974, patients with invasive cancer were routinely scheduled for abdominoperineal amputation, after which it was demonstrated that treatment with 5-fluorouracil and radiotherapy associated with mitomycin or capecitabine could be adequate to treat the tumour without surgery. Today, numerous studies have confirmed that combined multimodal treatment is effective and sufficient.
20世纪后半叶,肛门癌的发病率有所上升,其发病率比1992年至2001年这十年高出2.9%以上。然而,它在所有肛肠肿瘤中所占比例仍然较小,约为4%。其危险因素包括人乳头瘤病毒感染、性传播疾病史、外阴或宫颈癌病史、与人类免疫缺陷病毒感染相关或器官移植后的免疫抑制、血液学或免疫性疾病以及吸烟。最常见的症状是直肠出血(45%),其次是肛门疼痛和直肠肿物感。诊断需要进行临床检查、腹股沟淋巴结触诊、高分辨率肛门镜检查,随后进行细针穿刺活检或芯针活检。后续的组织学诊断以及盆腔淋巴结的计算机断层扫描或磁共振成像评估也是必要的。自1980年以来,被诊断为肛门癌的患者生存率有了显著提高。在欧洲,1983年至1994年期间,1年生存率从78%提高到81%,5年生存率提高了48%至54%。1974年以前,浸润性癌患者通常会接受腹会阴切除术,此后有研究表明,使用5-氟尿嘧啶和与丝裂霉素或卡培他滨联合的放疗可以在不进行手术的情况下充分治疗肿瘤。如今,大量研究证实联合多模式治疗是有效且充分的。