Department of Gastric Surgery, Sun Yat-sen University Cancer Center; State Key Laboratory of Oncology in South China; Collaborative Innovation Center for Cancer Medicine, Guangzhou, China.
Department of Psychiatry, The Third Affiliated Hospital, Sun Yat-sen University, No. 600 Tianhe Road, Guangzhou, China.
Biomed Res Int. 2020 May 6;2020:5059079. doi: 10.1155/2020/5059079. eCollection 2020.
To evaluate the efficacy of immuno-oncology combinational therapy (IOCT) versus monotherapy with programmed cell death 1 (PD-1) or PD-ligand 1 (PD-L1) inhibitors or conventional therapies, i.e., non-IOCT, in patients with advanced solid tumors.
We systematically searched the PubMed, Embase, and Cochrane Library databases from January 2015 to October 2018 for eligible studies. We included randomized trials of IOCT with available hazard ratios (HR) for death. The random effects model was used to calculate pooled HR for death; heterogeneity was assessed using statistics. The main outcome measure was overall survival (OS).
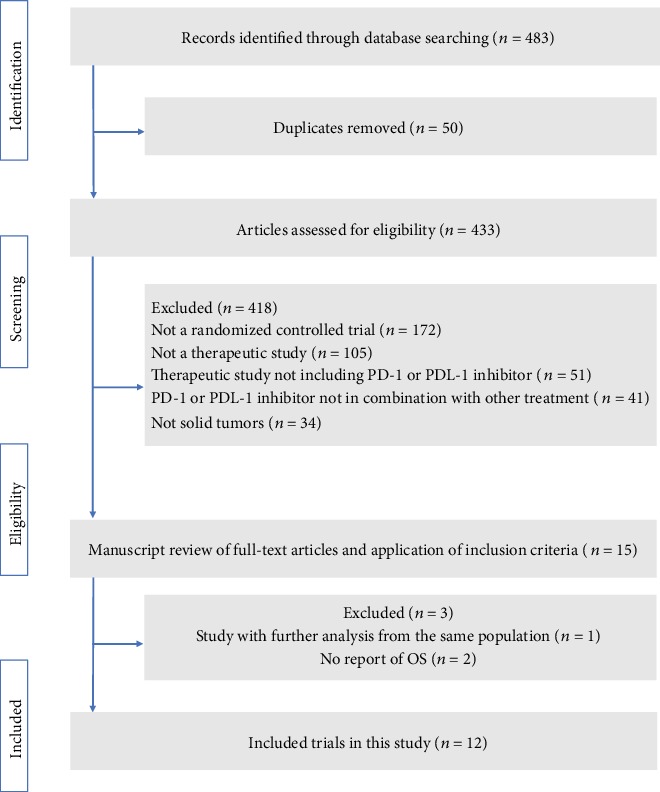
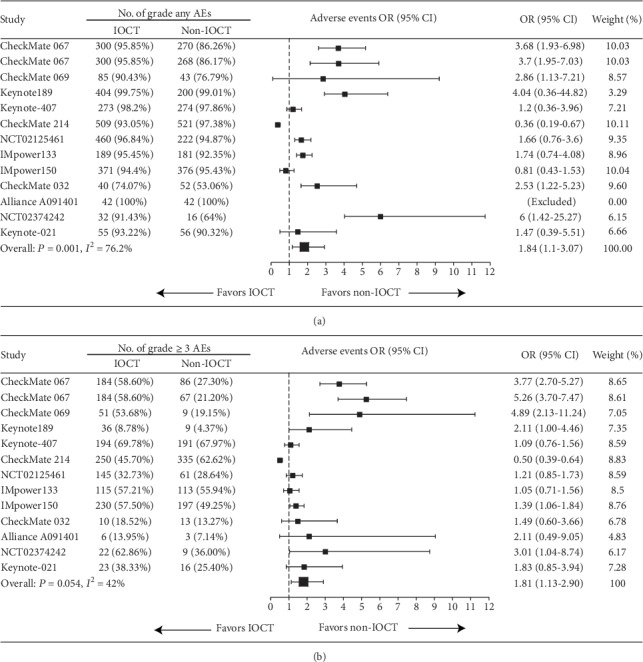
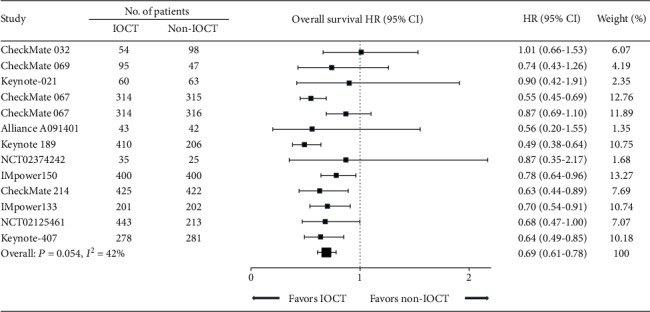
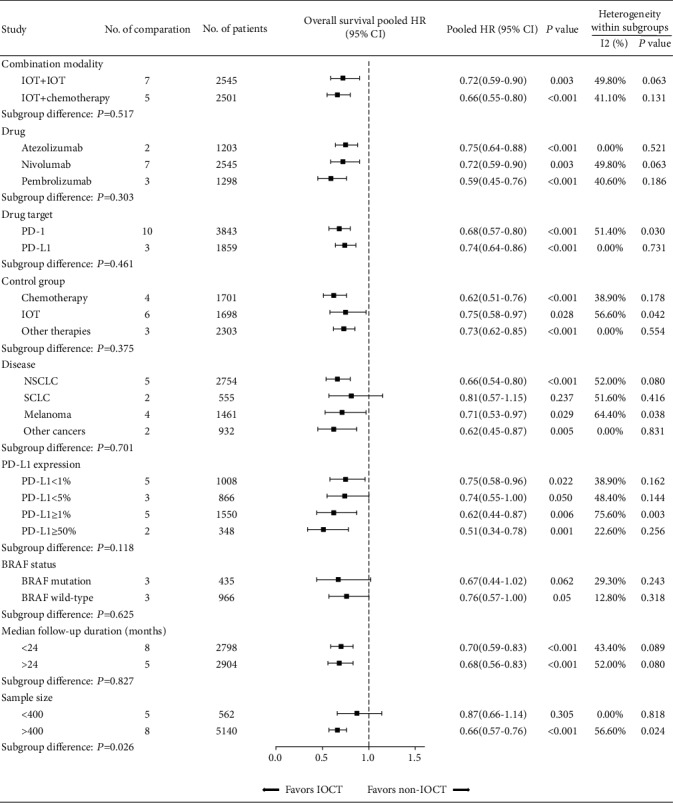
After screening 483 relevant articles, we identified twelve trials comprising 5388 patients for quantitative analysis. IOCT-treated patients had significantly higher tumor response rate (relative risk (RR): 2.51, 95% confidence interval (CI): 1.82-3.47), prolonged progression-free survival (HR 0.62, 95% CI: 0.53-0.74), and OS (HR 0.69, 95% CI: 0.61-0.78), compared with non-IOCT-treated patients. Sensitivity analyses also demonstrated the OS advantage of IOCT across different combination modalities, intervention agents, malignancy types, and PD-L1 expression (all < 0.05). Notably, there were higher odds of high-grade (grade ≥ 3) adverse events with IOCT (RR: 1.81, 95% CI: 1.13-2.90), but the risk of treatment-related death (RR: 1.16, 95% CI: 0.84-1.60) was not increased compared with non-IOCT.
IOCT is a preferable treatment option over PD-1/PD-L1 inhibitor monotherapy and conventional therapy for patients with advanced solid tumors. However, we should note the increased incidence rate of high-grade AEs in IOCT.
评估免疫肿瘤联合治疗(IOCT)与程序性细胞死亡 1(PD-1)或 PD-配体 1(PD-L1)抑制剂单药治疗或常规治疗(即非 IOCT)在晚期实体瘤患者中的疗效。
我们系统地检索了 PubMed、Embase 和 Cochrane Library 数据库,以获取 2015 年 1 月至 2018 年 10 月期间符合条件的研究。我们纳入了有可用死亡风险比(HR)的 IOCT 随机试验。使用随机效应模型计算死亡的汇总 HR;使用 统计量评估异质性。主要观察指标为总生存期(OS)。
在筛选了 483 篇相关文章后,我们确定了 12 项试验,共纳入了 5388 例患者进行定量分析。与非 IOCT 治疗患者相比,IOCT 治疗患者的肿瘤客观缓解率更高(相对风险(RR):2.51,95%置信区间(CI):1.82-3.47),无进展生存期更长(HR 0.62,95%CI:0.53-0.74),OS 也更长(HR 0.69,95%CI:0.61-0.78)。敏感性分析还表明,在不同的联合模式、干预药物、恶性肿瘤类型和 PD-L1 表达情况下,IOCT 均具有 OS 优势(均<0.05)。值得注意的是,IOCT 治疗相关不良事件(AE)的发生率更高(RR:1.81,95%CI:1.13-2.90),但与非 IOCT 相比,治疗相关死亡的风险(RR:1.16,95%CI:0.84-1.60)并未增加。
与 PD-1/PD-L1 抑制剂单药治疗或常规治疗相比,IOCT 是晚期实体瘤患者的更好治疗选择。然而,我们应该注意到 IOCT 中高等级 AE 的发生率增加。