Bassetti Matteo, Vena Antonio, Giacobbe Daniele Roberto, Falcone Marco, Tiseo Giusy, Giannella Maddalena, Pascale Renato, Meschiari Marianna, Digaetano Margherita, Oliva Alessandra, Rovelli Cristina, Carannante Novella, Losito Angela Raffaella, Carbonara Sergio, Mariani Michele Fabiano, Mastroianni Antonio, Angarano Gioacchino, Tumbarello Mario, Tascini Carlo, Grossi Paolo, Mastroianni Claudio Maria, Mussini Cristina, Viale Pierluigi, Menichetti Francesco, Viscoli Claudio, Russo Alessandro
Department of Health Sciences, University of Genoa, Genoa, Italy.
Department of Clinical and Experimental Medicine, University of Pisa, Pisa, Italy.
Open Forum Infect Dis. 2020 Apr 21;7(5):ofaa139. doi: 10.1093/ofid/ofaa139. eCollection 2020 May.
Few data are reported in the literature about the outcome of patients with severe extended-spectrum β-lactamase-producing (ESBL-E) infections treated with ceftolozane/tazobactam (C/T), in empiric or definitive therapy.
A multicenter retrospective study was performed in Italy (June 2016-June 2019). Successful clinical outcome was defined as complete resolution of clinical signs/symptoms related to ESBL-E infection and lack of microbiological evidence of infection. The primary end point was to identify predictors of clinical failure of C/T therapy.
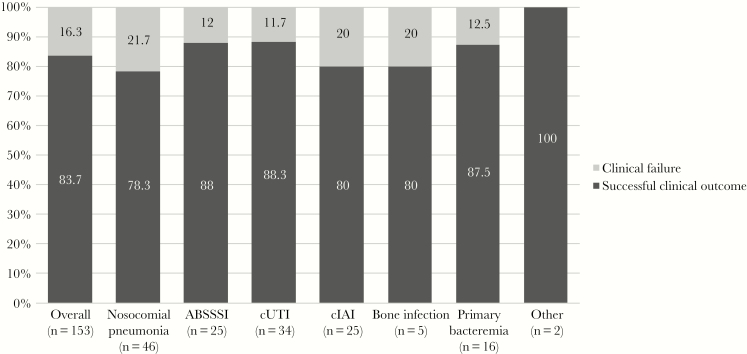
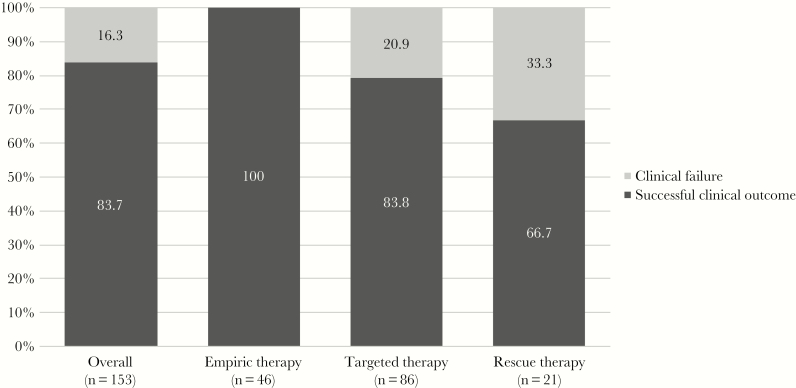
C/T treatment was documented in 153 patients: pneumonia was the most common diagnosis (n = 46, 30%), followed by 34 cases of complicated urinary tract infections (22.2%). Septic shock was observed in 42 (27.5%) patients. C/T was used as empiric therapy in 46 (30%) patients and as monotherapy in 127 (83%) patients. Favorable clinical outcome was observed in 128 (83.7%) patients; 25 patients were considered to have failed C/T therapy. Overall, 30-day mortality was reported for 15 (9.8%) patients. At multivariate analysis, Charlson comorbidity index >4 (odds ratio [OR], 2.3; 95% confidence interval [CI], 1.9-3.5; = .02), septic shock (OR, 6.2; 95% CI, 3.8-7.9; < .001), and continuous renal replacement therapy (OR, 3.1; 95% CI, 1.9-5.3; = .001) were independently associated with clinical failure, whereas empiric therapy displaying in vitro activity (OR, 0.12; 95% CI, 0.01-0.34; < .001) and adequate source control of infection (OR, 0.42; 95% CI, 0.14-0.55; < .001) were associated with clinical success.
Data show that C/T could be a valid option in empiric and/or targeted therapy in patients with severe infections caused by ESBL-producing . Clinicians should be aware of the risk of clinical failure with standard-dose C/T therapy in septic patients receiving CRRT.
关于接受头孢洛扎/他唑巴坦(C/T)治疗的产超广谱β-内酰胺酶(ESBL-E)严重感染患者的治疗结果,文献报道的数据较少,无论是经验性治疗还是确定性治疗。
在意大利进行了一项多中心回顾性研究(2016年6月至2019年6月)。成功的临床结局定义为与ESBL-E感染相关的临床体征/症状完全缓解且缺乏感染的微生物学证据。主要终点是确定C/T治疗临床失败的预测因素。
153例患者接受了C/T治疗:肺炎是最常见的诊断(n = 46,30%),其次是34例复杂性尿路感染(22.2%)。42例(27.5%)患者发生感染性休克。46例(30%)患者将C/T用作经验性治疗,127例(83%)患者将其用作单一疗法。128例(83.7%)患者临床结局良好;25例患者被认为C/T治疗失败。总体而言,15例(9.8%)患者报告了30天死亡率。多因素分析显示,Charlson合并症指数>4(比值比[OR],2.3;95%置信区间[CI],1.9 - 3.5;P = .02)、感染性休克(OR,6.2;95% CI,3.8 - 7.9;P < .001)和持续肾脏替代治疗(OR,3.1;95% CI,1.9 - 5.3;P = .001)与临床失败独立相关,而具有体外活性的经验性治疗(OR,0.12;95% CI,0.01 - 0.34;P < .001)和充分的感染源控制(OR,0.42;95% CI,0.14 - 0.55;P < .001)与临床成功相关。
数据表明,C/T可能是产ESBL-E严重感染患者经验性和/或靶向治疗的有效选择。临床医生应意识到在接受CRRT的脓毒症患者中,标准剂量C/T治疗存在临床失败的风险。