Barbier François, Hraiech Sami, Kernéis Solen, Veluppillai Nathanaël, Pajot Olivier, Poissy Julien, Roux Damien, Zahar Jean-Ralph
Médecine Intensive Réanimation, Centre Hospitalier Régional d'Orléans, 14, Avenue de l'Hôpital, 45000, Orléans, France.
Institut Maurice Rapin, Hôpital Henri Mondor, Créteil, France.
Ann Intensive Care. 2023 Jul 18;13(1):65. doi: 10.1186/s13613-023-01153-6.
Healthcare-associated infections involving Gram-negative bacteria (GNB) with difficult-to-treat resistance (DTR) phenotype are associated with impaired patient-centered outcomes and poses daily therapeutic challenges in most of intensive care units worldwide. Over the recent years, four innovative β-lactam/β-lactamase inhibitor (BL/BLI) combinations (ceftolozane-tazobactam, ceftazidime-avibactam, imipenem-relebactam and meropenem-vaborbactam) and a new siderophore cephalosporin (cefiderocol) have been approved for the treatment of certain DTR-GNB infections. The literature addressing their microbiological spectrum, pharmacokinetics, clinical efficacy and safety was exhaustively audited by our group to support the recent guidelines of the French Intensive Care Society on their utilization in critically ill patients. This narrative review summarizes the available evidence and unanswered questions on these issues.
A systematic search for English-language publications in PUBMED and the Cochrane Library database from inception to November 15, 2022.
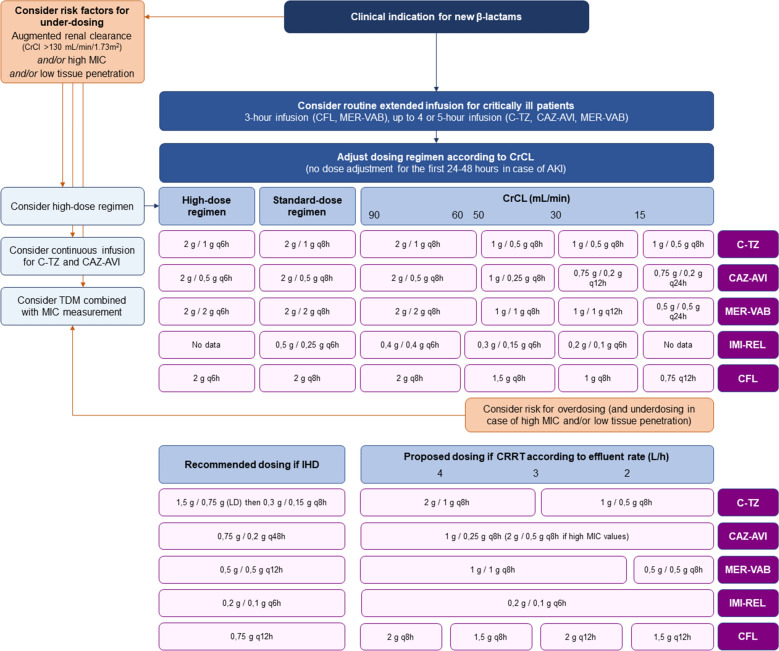
These drugs have demonstrated relevant clinical success rates and a reduced renal risk in most of severe infections for whom polymyxin- and/or aminoglycoside-based regimen were historically used as last-resort strategies-namely, ceftazidime-avibactam for infections due to Klebsiella pneumoniae carbapenemase (KPC)- or OXA-48-like-producing Enterobacterales, meropenem-vaborbactam for KPC-producing Enterobacterales, ceftazidime-avibactam/aztreonam combination or cefiderocol for metallo-β-lactamase (MBL)-producing Enterobacterales, and ceftolozane-tazobactam, ceftazidime-avibactam and imipenem-relebactam for non-MBL-producing DTR Pseudomonas aeruginosa. However, limited clinical evidence exists in critically ill patients. Extended-infusion scheme (except for imipenem-relebactam) may be indicated for DTR-GNB with high minimal inhibitory concentrations and/or in case of augmented renal clearance. The potential benefit of combining these agents with other antimicrobials remains under-investigated, notably for the most severe presentations. Other important knowledge gaps include pharmacokinetic information in particular situations (e.g., pneumonia, other deep-seated infections, and renal replacement therapy), the hazard of treatment-emergent resistance and possible preventive measures, the safety of high-dose regimen, the potential usefulness of rapid molecular diagnostic tools to rationalize their empirical utilization, and optimal treatment durations. Comparative clinical, ecological, and medico-economic data are needed for infections in whom two or more of these agents exhibit in vitro activity against the causative pathogen.
New BL/BLI combinations and cefiderocol represent long-awaited options for improving the management of DTR-GNB infections. Several research axes must be explored to better define the positioning and appropriate administration scheme of these drugs in critically ill patients.
涉及具有难治疗耐药(DTR)表型的革兰氏阴性菌(GNB)的医疗保健相关感染与以患者为中心的预后受损相关,并且在全球大多数重症监护病房中构成日常治疗挑战。近年来,四种新型β-内酰胺/β-内酰胺酶抑制剂(BL/BLI)组合(头孢洛扎坦-他唑巴坦、头孢他啶-阿维巴坦、亚胺培南-瑞来巴坦和美罗培南-瓦泊巴坦)以及一种新型铁载体头孢菌素(头孢地尔)已被批准用于治疗某些DTR-GNB感染。我们团队详尽审核了关于它们的微生物谱、药代动力学、临床疗效和安全性的文献,以支持法国重症监护学会近期关于在重症患者中使用这些药物的指南。本叙述性综述总结了关于这些问题的现有证据和未解答的问题。
在PUBMED和Cochrane图书馆数据库中对从创建到2022年11月15日的英文出版物进行系统检索。
这些药物在大多数严重感染中已显示出相关的临床成功率并降低了肾脏风险,对于这些严重感染,基于多粘菌素和/或氨基糖苷类的方案在历史上曾被用作最后手段策略——即,头孢他啶-阿维巴坦用于治疗由肺炎克雷伯菌碳青霉烯酶(KPC)或产OXA-48样酶的肠杆菌科细菌引起的感染,美罗培南-瓦泊巴坦用于治疗产KPC的肠杆菌科细菌,头孢他啶-阿维巴坦/氨曲南组合或头孢地尔用于治疗产金属β-内酰胺酶(MBL)的肠杆菌科细菌,以及头孢洛扎坦-他唑巴坦、头孢他啶-阿维巴坦和亚胺培南-瑞来巴坦用于治疗非产MBL的DTR铜绿假单胞菌。然而,重症患者中的临床证据有限。对于最低抑菌浓度高和/或肾脏清除率增加的DTR-GNB,可能需要延长输注方案(亚胺培南-瑞来巴坦除外)。将这些药物与其他抗菌药物联合使用的潜在益处仍研究不足,尤其是对于最严重的病例。其他重要的知识空白包括特殊情况下的药代动力学信息(例如,肺炎、其他深部感染和肾脏替代治疗)、治疗后出现耐药的风险和可能的预防措施、高剂量方案的安全性、快速分子诊断工具对其经验性使用进行合理化的潜在效用以及最佳治疗持续时间。对于两种或更多种这些药物对病原体具有体外活性的感染,需要比较临床、生态学和药物经济学数据。
新型BL/BLI组合和头孢地尔是改善DTR-GNB感染管理的期待已久的选择。必须探索几个研究方向,以更好地确定这些药物在重症患者中的定位和适当给药方案。