Division of Surgical Oncology, Winship Cancer Institute, Emory University, Atlanta, Georgia.
Bioinformatics and Biostatistics Shared Resource, Winship Cancer Institute, Emory University, Atlanta, Georgia.
J Surg Oncol. 2020 Sep;122(3):457-468. doi: 10.1002/jso.25976. Epub 2020 May 29.
For pancreatic adenocarcinoma (PDAC), no studies have established any association between earlier treatment initiation and long-term outcomes. In addition, an optimal type of initial treatment for the localized disease remains ill-defined.
Patients in the National Cancer Database (2004-2015) with clinical stage I (CS-I) and II (CS-II) PDAC who underwent curative-intent resection were included. Optimal time from diagnosis-to-treatment including neoadjuvant chemotherapy, neoadjuvant chemoradiation, or upfront surgery was assessed. An optimal type of treatment was evaluated. The primary outcome was overall survival (OS).
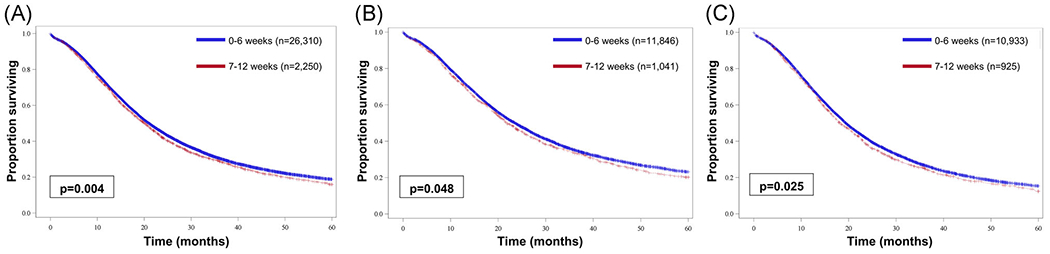
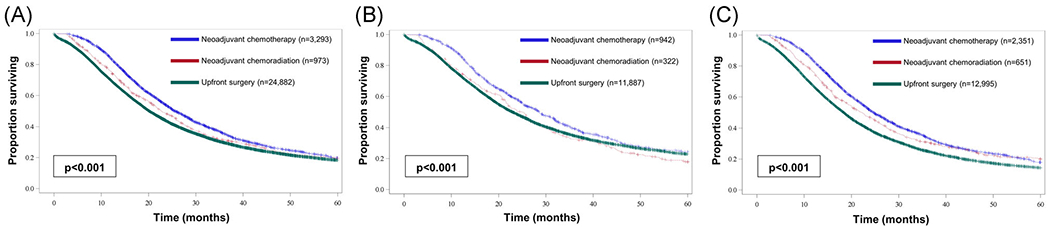
Among 29 167 patients, starting any treatment within 0 to 6 weeks was associated with improved median OS compared with 7 to 12 weeks (21.0 vs 20.1 months; P = .004). This persisted when accounting for sex, race, and Charlson-Deyo score (hazard ratio [HR], 0.94; P = 0.02) and on subset analysis for CS-I (23.5 vs 21.8 months; P = .04) and CS-II (19.4 vs 18.3 months; P = .03). Neoadjuvant chemotherapy was associated with improved OS compared with neoadjuvant chemoradiation (25.6 vs 22.7 months; P < .0001) or US (25.6 vs 20.1 months; P < .0001) even when accounting for sex, race, and Charlson-Deyo score (neoadjuvant chemoradiation: HR, 0.86; P < .001; US: HR, 0.79; P < .001). This improvement persisted in subset analysis with NC compared with neoadjuvant chemoradiation (CS-I: 28.6 vs 25.0 months; CS-II: 25.0 vs 22.9 months; both P < .0001) and to US (CS-I: 28.6 vs 22.9 months; CS-II: 24.7 vs 18.4 months; both P < .0001). On multivariable analysis for each CS-I/CS-II, NC remained associated with 20% improved survival compared with neoadjuvant chemoradiation or upfront surgery.
For PDAC, initiation of therapy within 6 weeks from diagnosis is associated with improved survival, with neoadjuvant chemotherapy associated with the best survival compared with neoadjuvant chemoradiation or upfront surgery.
对于胰腺导管腺癌(PDAC),尚无研究确定更早开始治疗与长期结局之间存在关联。此外,局部疾病的最佳初始治疗类型仍未明确。
本研究纳入了国家癌症数据库(2004-2015 年)中接受根治性手术治疗的临床分期 I(CS-I)和 II(CS-II)期 PDAC 患者。评估了从诊断到治疗(包括新辅助化疗、新辅助放化疗或直接手术)的最佳时间。评估了最佳治疗类型。主要结局是总生存期(OS)。
在 29167 例患者中,与 7-12 周相比,0-6 周内开始任何治疗均与中位 OS 改善相关(21.0 个月 vs 20.1 个月;P=0.004)。当考虑到性别、种族和 Charlson-Deyo 评分(风险比[HR],0.94;P=0.02)以及 CS-I(23.5 个月 vs 21.8 个月;P=0.04)和 CS-II(19.4 个月 vs 18.3 个月;P=0.03)亚组分析时,这种相关性仍然存在。与新辅助放化疗(25.6 个月 vs 22.7 个月;P<0.0001)或直接手术(25.6 个月 vs 20.1 个月;P<0.0001)相比,新辅助化疗与 OS 改善相关,即使考虑到性别、种族和 Charlson-Deyo 评分(新辅助放化疗:HR,0.86;P<0.001;直接手术:HR,0.79;P<0.001)。与新辅助放化疗相比,这种改善在 NC 与 CS-I(28.6 个月 vs 25.0 个月;CS-II:25.0 个月 vs 22.9 个月;均 P<0.0001)和直接手术(CS-I:28.6 个月 vs 22.9 个月;CS-II:24.7 个月 vs 18.4 个月;均 P<0.0001)的亚组分析中仍然存在。在每个 CS-I/CS-II 的多变量分析中,与新辅助放化疗或直接手术相比,NC 与 20%的生存改善相关。
对于 PDAC,从诊断到开始治疗的时间在 6 周内与生存改善相关,与新辅助放化疗或直接手术相比,新辅助化疗与最佳生存相关。