Division of General and Transplant Surgery, University of Pisa, Via Savi 10, 56126, Pisa, PI, Italy.
College of Medicine and Public Health, Flinders University, Adelaide, South Australia, Australia.
Updates Surg. 2024 Sep;76(5):1573-1591. doi: 10.1007/s13304-024-01860-0. Epub 2024 Apr 29.
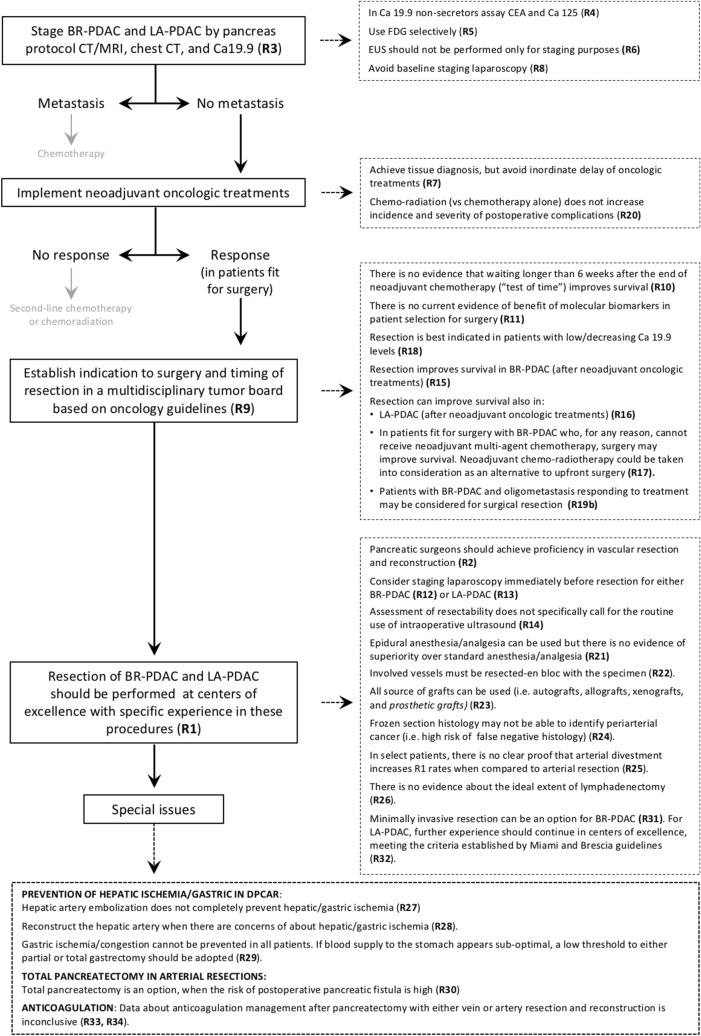
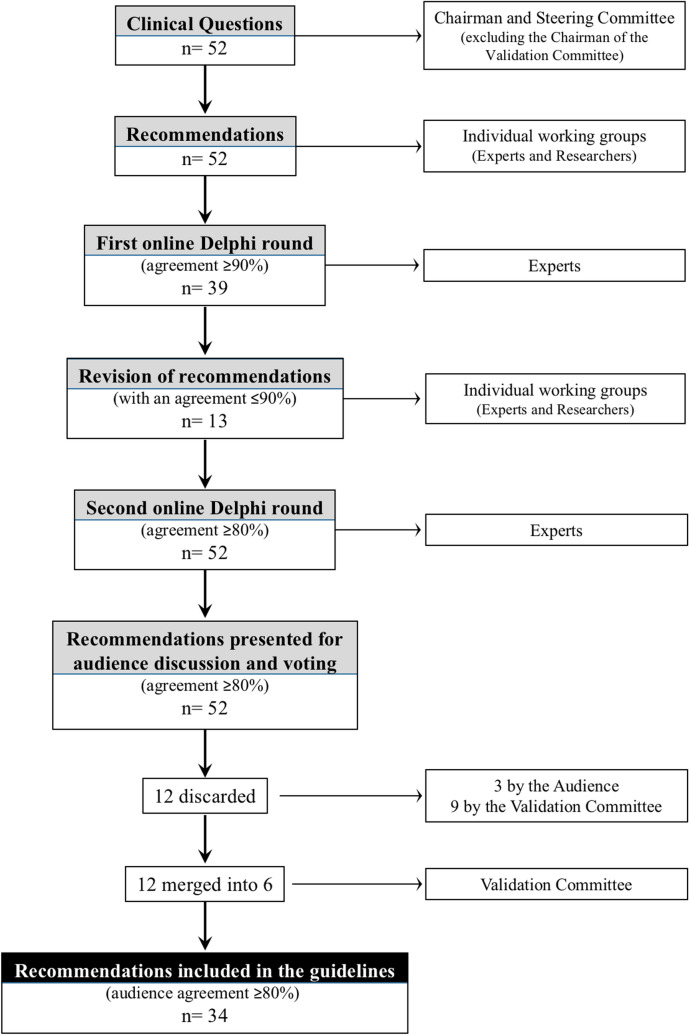
The REDISCOVER guidelines present 34 recommendations for the selection and perioperative care of borderline-resectable (BR-PDAC) and locally advanced ductal adenocarcinoma of the pancreas (LA-PDAC). These guidelines represent a significant shift from previous approaches, prioritizing tumor biology over anatomical features as the primary indication for resection. Condensed herein, they provide a practical management algorithm for clinical practice. However, the guidelines also highlight the need to redefine LA-PDAC to align with modern treatment strategies and to solve some contradictions within the current definition, such as grouping "difficult" and "impossible" to resect tumors together. Furthermore, the REDISCOVER guidelines highlight several areas requiring urgent research. These include the resection of the superior mesenteric artery, the management strategies for patients with LA-PDAC who are fit for surgery but unable to receive multi-agent neoadjuvant chemotherapy, the approach to patients with LA-PDAC who are fit for surgery but demonstrate high serum Ca 19.9 levels even after neoadjuvant treatment, and the optimal timing and number of chemotherapy cycles prior to surgery. Additionally, the role of primary chemoradiotherapy versus chemotherapy alone in LA-PDAC, the timing of surgical resection post-neoadjuvant/primary chemoradiotherapy, the efficacy of ablation therapies, and the management of oligometastasis in patients with LA-PDAC warrant investigation. Given the limited evidence for many issues, refining existing management strategies is imperative. The establishment of the REDISCOVER registry ( https://rediscover.unipi.it/ ) offers promise of a unified research platform to advance understanding and improve the management of BR-PDAC and LA-PDAC.
RECOVER 指南提出了 34 项关于边界可切除(BR-PDAC)和局部进展期胰腺导管腺癌(LA-PDAC)的选择和围手术期护理的建议。这些指南代表了从以前的方法的重大转变,优先考虑肿瘤生物学而不是解剖特征作为切除的主要指征。本文浓缩了它们为临床实践提供了一种实用的管理算法。然而,这些指南还强调需要重新定义 LA-PDAC,以与现代治疗策略保持一致,并解决当前定义中的一些矛盾,例如将“困难”和“不可能”切除的肿瘤归为一组。此外,RECOVER 指南强调了几个需要紧急研究的领域。这些包括肠系膜上动脉的切除,适合手术但无法接受多药新辅助化疗的 LA-PDAC 患者的管理策略,适合手术但在新辅助治疗后血清 Ca 19.9 水平仍然升高的 LA-PDAC 患者的治疗方法,以及手术前化疗的最佳时机和周期数。此外,LA-PDAC 中原发放化疗与单纯化疗的作用、新辅助/原发放化疗后手术切除的时机、消融治疗的疗效以及 LA-PDAC 中寡转移的处理都需要进一步研究。鉴于许多问题的证据有限,细化现有的管理策略是当务之急。建立 RECOVER 登记处(https://rediscover.unipi.it/)有望为统一的研究平台提供支持,以推进对 BR-PDAC 和 LA-PDAC 的认识并改善其管理。