Emergency and Critical Care Medicine, St. Luke's International Hospital, Tokyo, Japan.
Emergency and Critical Care Medicine, St. Luke's International Hospital, Tokyo, Japan.
Am J Emerg Med. 2020 Oct;38(10):2243.e1-2243.e3. doi: 10.1016/j.ajem.2020.05.042. Epub 2020 May 22.
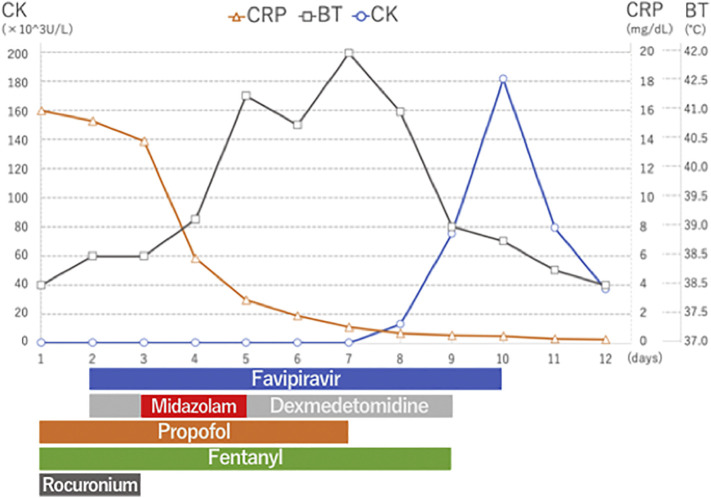
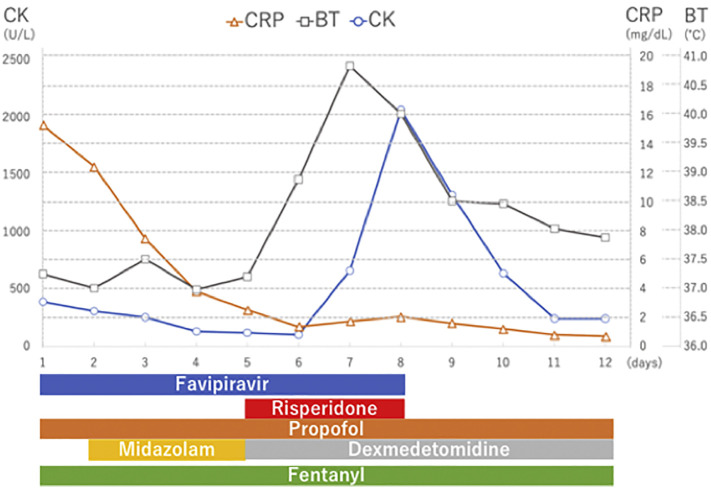
We report the first two cases of Coronavirus Disease 2019 (COVID-19) who were receiving intensive care including favipiravir, and were clinically diagnosed with neuroleptic malignant syndrome (NMS) to focus attention on NMS in COVID-19 management. Case 1: A 46-year-old-man with acute respiratory distress syndrome (ARDS) caused by COVID-19 infection was being administered favipiravir. Fentanyl, propofol, and rocuronium were also given. On day 3, midazolam administration was initiated for deep sedation. On day 5, his high body temperature increased to 41.2 °C, creatine kinase level elevated, and he developed tachycardia, tachypnea, altered consciousness, and diaphoresis. NMS was suspected, and supportive therapy was initiated. High-grade fever persisted for 4 days and subsided on day 9. Case 2: A 44-year-old-man with ARDS caused by COVID-19 infection was being treated with favipiravir. On day 5, risperidone was started for delirium. On day 7, his body temperature suddenly increased to 40.8 °C, his CK level elevated, and he developed tachycardia, tachypnea, altered consciousness, and diaphoresis. NMS diagnosis was confirmed, and both, favipiravir and risperidone were discontinued on day 8. On the same day, his CK levels decreased, and his body temperature normalized on day 9. Patients with COVID-19 infection frequently require deep sedation and develop delirium; therefore, more attention should be paid to the development of NMS in patients who are being administered such causative agents. The mechanism underlying the occurrence of NMS in COVID-19 patients treated with favipiravir remains unknown. Therefore, careful consideration of NMS development is necessary in the management of COVID-19 patients.
我们报告了首例 2 例接受包括法匹拉韦在内的重症监护的 2019 年冠状病毒病(COVID-19)患者,临床诊断为神经阻滞剂恶性综合征(NMS),以引起人们对 COVID-19 管理中 NMS 的关注。病例 1:一名 46 岁男性因 COVID-19 感染导致急性呼吸窘迫综合征(ARDS),正在接受法匹拉韦治疗。还给予了芬太尼、丙泊酚和罗库溴铵。第 3 天开始给予咪达唑仑进行深度镇静。第 5 天,他的高热升至 41.2°C,肌酸激酶水平升高,并出现心动过速、呼吸急促、意识改变和出汗。怀疑发生 NMS,并开始给予支持性治疗。高热持续了 4 天,第 9 天消退。病例 2:一名 44 岁男性因 COVID-19 感染导致 ARDS,正在接受法匹拉韦治疗。第 5 天,开始使用利培酮治疗谵妄。第 7 天,他的体温突然升高至 40.8°C,肌酸激酶水平升高,并出现心动过速、呼吸急促、意识改变和出汗。确诊为 NMS,并于第 8 天停用法匹拉韦和利培酮。同日,他的 CK 水平下降,第 9 天体温恢复正常。COVID-19 感染患者经常需要深度镇静并出现谵妄;因此,在给予此类致病药物的患者中,应更加注意 NMS 的发生。法匹拉韦治疗的 COVID-19 患者发生 NMS 的机制尚不清楚。因此,在 COVID-19 患者的管理中,需要仔细考虑 NMS 的发生。