Rispoli Marco, Nespoli Moana Rossella, Mattiacci Dario Maria, Curcio Carlo, Casazza Dino, Amore Dario
Monaldi Hospital, Naples, Italy.
Int J Surg Case Rep. 2020;71:294-296. doi: 10.1016/j.ijscr.2020.04.097. Epub 2020 May 17.
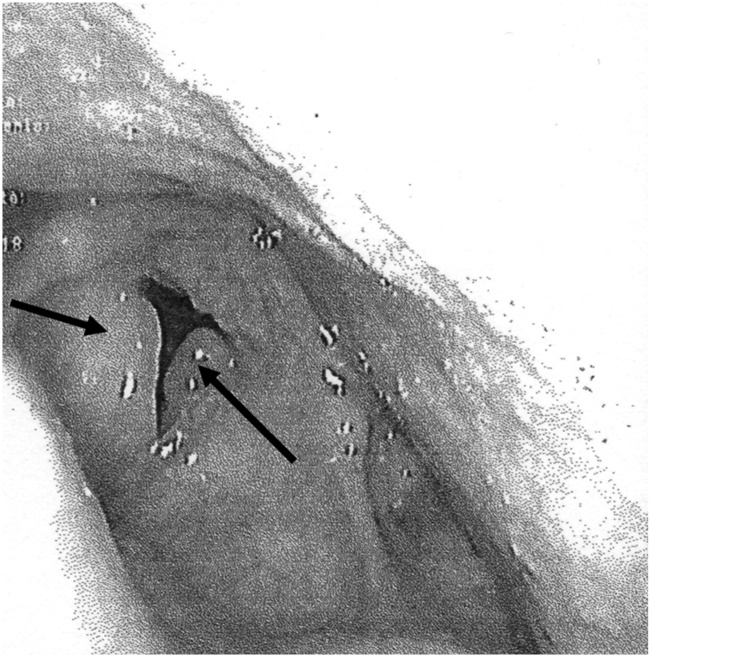
Reinke's edema (RE) is a benign laryngeal disease. We describe the case of a patient with history of bilateral RE requiring surgical treatment, that came to our attention for a lung lobectomy due to adenocarcinoma. In consideration of the possible complications at the time of extubation and of the probable difficult control of the airways, the patient underwent intervention of microflap surgery for the RE at the same time of lobectomy. We opted for Bronchial Blocker (BB) using a Viva-sight™ Single Lumen Tube (SLT) Internal Diameter (ID) 7.0 mm (Ambu A/S, Baltorpbakken 13, DK-2750 Ballerup, Denmark) with integrated high-resolution camera.
The patient (female, 67 years old, BMI 28) was a candidate for lung lobectomy. She reported a RE requiring surgical treatment. An armoured Endo Tracheal Tube (ETT) ID 5.0 mm was positioned and microflap surgery was performed. Once this surgery ended, the armoured ETT was removed after placing an airway guide wire exchanger and a SLT ID 7.0 mm was placed. VivaSight-endoblocher™ (EB) was positioned in the right bronchus.
We opted for double intervention, the risk that could result from the delay persuaded the patient to perform surgery for the RE. Postponing the lobectomy was dangerous for the oncological situation. The Viva-Sight SLT represented the right compromise.
Even after the microflap, the space available for the ETT was reduced and, in order not to traumatize a tissue already stressed by surgery and to facilitate the tracheal intubation, we opted for BB using a Viva-sight™.
莱因克水肿(RE)是一种良性喉部疾病。我们描述了一例有双侧RE病史且需要手术治疗的患者,该患者因腺癌前来我院接受肺叶切除术。考虑到拔管时可能出现的并发症以及气道可能难以控制,该患者在肺叶切除的同时接受了RE的微瓣手术干预。我们选择使用内径7.0毫米的Viva-sight™单腔管(SLT)(丹麦阿迈斯公司,巴勒鲁普市巴尔托普巴肯13号,邮编DK - 2750)并集成高分辨率摄像头的支气管封堵器(BB)。
患者(女性,67岁,BMI 28)是肺叶切除术的候选者。她有需要手术治疗的RE病史。放置了一根内径5.0毫米的钢丝加强型气管内导管(ETT)并进行了微瓣手术。该手术结束后,在放置气道导丝交换器后移除了钢丝加强型ETT,并放置了一根内径7.0毫米的SLT。VivaSight - 支气管封堵器™(EB)放置在右支气管。
我们选择了双重干预,延迟手术可能带来的风险促使患者进行RE手术。推迟肺叶切除术对肿瘤病情不利。Viva - Sight SLT是合适的折衷选择。
即使在微瓣手术后,可供ETT使用的空间也减小了,为了不损伤已经因手术而受压的组织并便于气管插管,我们选择使用Viva - sight™进行BB。