Department of Psychiatry and Psychotherapy, Medical University of Vienna, Vienna, Austria.
Section on Neurobiology and Treatment of Mood Disorders, Intramural Research Program, National Institute of Mental Health, National Institutes of Health, Bethesda, MD, USA.
Transl Psychiatry. 2019 Apr 3;9(1):127. doi: 10.1038/s41398-019-0460-3.
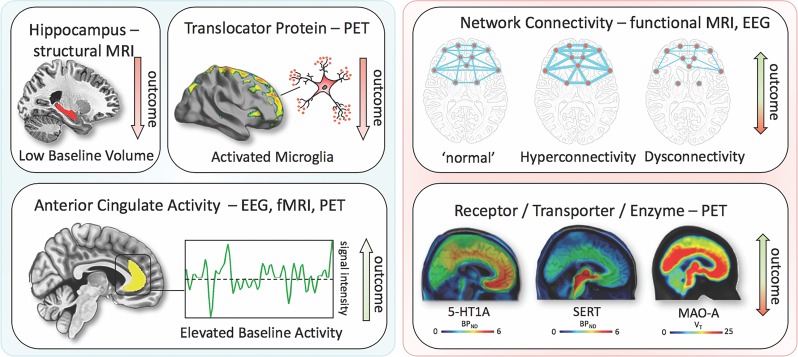
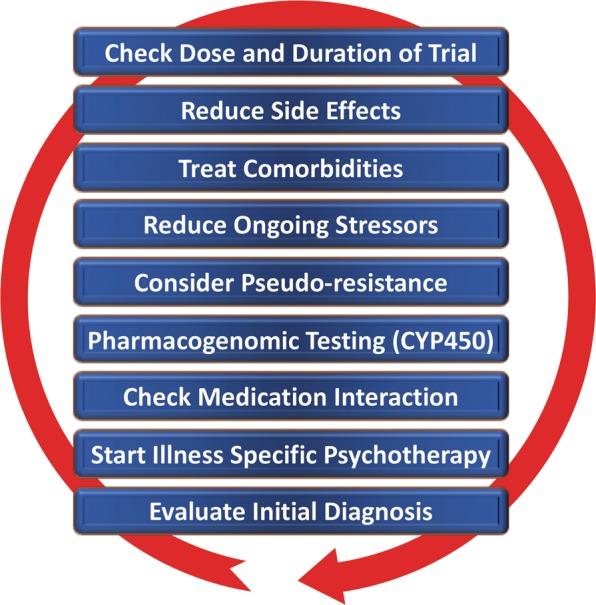
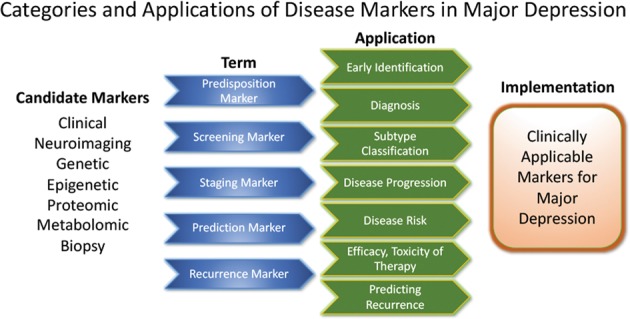
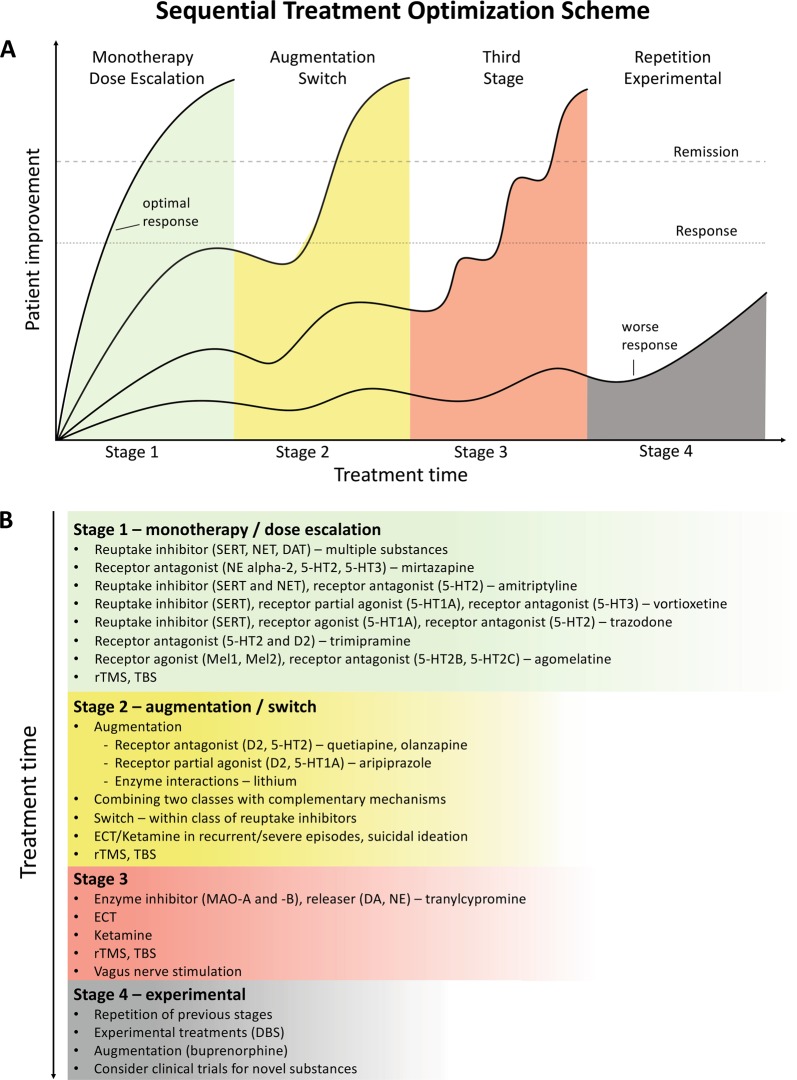
Treatment outcomes for major depressive disorder (MDD) need to be improved. Presently, no clinically relevant tools have been established for stratifying subgroups or predicting outcomes. This literature review sought to investigate factors closely linked to outcome and summarize existing and novel strategies for improvement. The results show that early recognition and treatment are crucial, as duration of untreated depression correlates with worse outcomes. Early improvement is associated with response and remission, while comorbidities prolong course of illness. Potential biomarkers have been explored, including hippocampal volumes, neuronal activity of the anterior cingulate cortex, and levels of brain-derived neurotrophic factor (BDNF) and central and peripheral inflammatory markers (e.g., translocator protein (TSPO), interleukin-6 (IL-6), C-reactive protein (CRP), tumor necrosis factor alpha (TNFα)). However, their integration into routine clinical care has not yet been fully elucidated, and more research is needed in this regard. Genetic findings suggest that testing for CYP450 isoenzyme activity may improve treatment outcomes. Strategies such as managing risk factors, improving clinical trial methodology, and designing structured step-by-step treatments are also beneficial. Finally, drawing on existing guidelines, we outline a sequential treatment optimization paradigm for selecting first-, second-, and third-line treatments for acute and chronically ill patients. Well-established treatments such as electroconvulsive therapy (ECT) are clinically relevant for treatment-resistant populations, and novel transcranial stimulation methods such as theta-burst stimulation (TBS) and magnetic seizure therapy (MST) have shown promising results. Novel rapid-acting antidepressants, such as ketamine, may also constitute a paradigm shift in treatment optimization for MDD.
治疗重度抑郁症(MDD)的效果有待改善。目前,尚未建立用于分层亚组或预测结果的有临床意义的工具。本文综述旨在探讨与结局密切相关的因素,并总结现有的和新的改善策略。结果表明,早期识别和治疗至关重要,因为未治疗的抑郁持续时间与较差的结局相关。早期改善与反应和缓解相关,而合并症则延长了疾病的病程。已经探索了潜在的生物标志物,包括海马体积、前扣带皮层的神经元活动以及脑源性神经营养因子(BDNF)和中枢及外周炎症标志物(如转位蛋白(TSPO)、白细胞介素-6(IL-6)、C 反应蛋白(CRP)、肿瘤坏死因子-α(TNFα))的水平。然而,它们尚未完全纳入常规临床护理,在这方面还需要更多的研究。遗传研究结果表明,检测 CYP450 同工酶活性可能改善治疗效果。管理危险因素、改善临床试验方法和设计结构化的逐步治疗策略等策略也有益。最后,我们参考现有的指南,为急性和慢性患者的一线、二线和三线治疗选择勾勒出一个序贯治疗优化范例。电惊厥治疗(ECT)等成熟的治疗方法对治疗抵抗人群具有临床意义,而新型经颅刺激方法,如 theta 爆发刺激(TBS)和磁惊厥治疗(MST)已显示出良好的效果。新型快速作用抗抑郁药,如氯胺酮,也可能构成 MDD 治疗优化的范式转变。