Massachusetts General Hospital Cancer Center, Massachusetts General Hospital and Harvard Medical School, Boston, Massachusetts, USA.
Department of Neurology, Massachusetts General Hospital and Harvard Medical School, Boston, Massachusetts, USA.
Oncologist. 2020 Aug;25(8):e1221-e1232. doi: 10.1634/theoncologist.2020-0085. Epub 2020 Jun 18.
Pseudoprogression (PP) and treatment-induced brain tissue necrosis (TN) are challenging cancer treatment-related effects. Both phenomena remain insufficiently defined; differentiation from recurrent disease frequently necessitates tissue biopsy. We here characterize distinctive features of PP and TN to facilitate noninvasive diagnosis and clinical management.
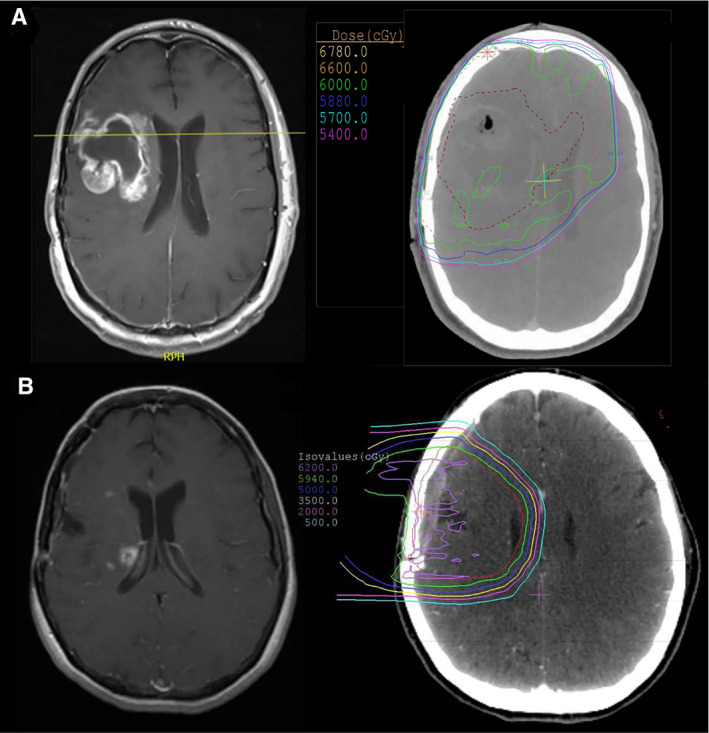
Patients with glioma and confirmed PP (defined as appearance <5 months after radiotherapy [RT] completion) or TN (>5 months after RT) were retrospectively compared using clinical, radiographic, and histopathological data. Each imaging event/lesion (region of interest [ROI]) diagnosed as PP or TN was longitudinally evaluated by serial imaging.
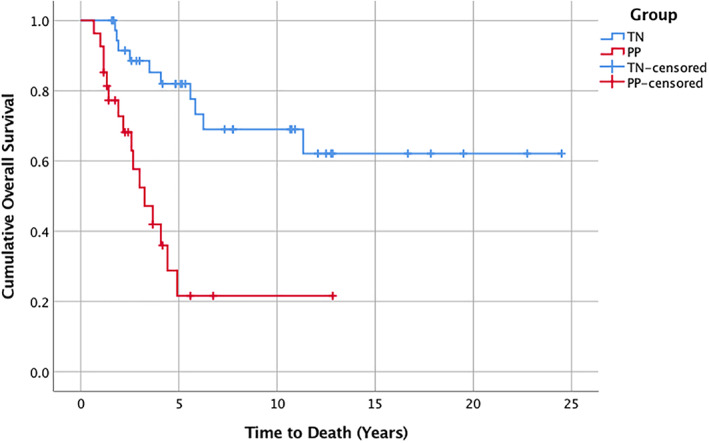
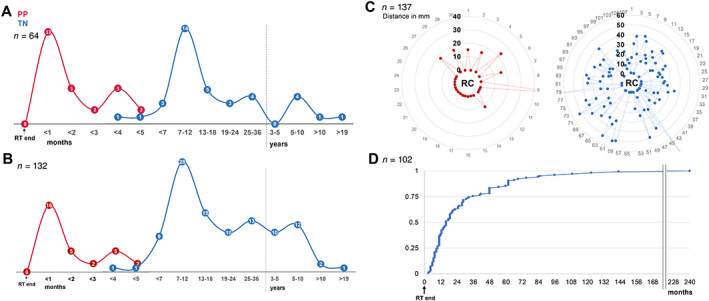
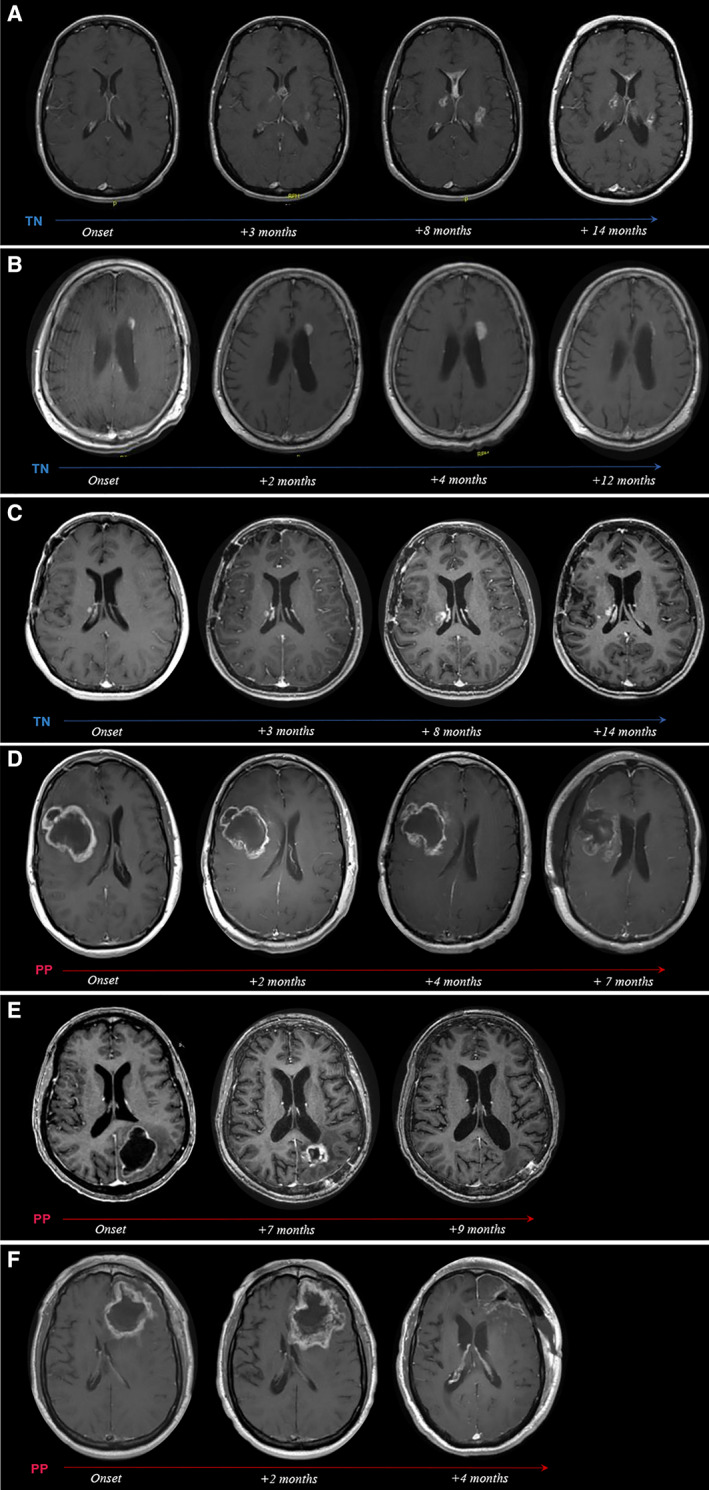
We identified 64 cases of mostly (80%) biopsy-confirmed PP (n = 27) and TN (n = 37), comprising 137 ROIs in total. Median time of onset for PP and TN was 1 and 11 months after RT, respectively. Clinically, PP occurred more frequently during active antineoplastic treatment, necessitated more steroid-based interventions, and was associated with glioblastoma (81 vs. 40%), fewer IDH1 mutations, and shorter median overall survival. Radiographically, TN lesions often initially manifested periventricularly (n = 22/37; 60%), were more numerous (median, 2 vs. 1 ROIs), and contained fewer malignant elements upon biopsy. By contrast, PP predominantly developed around the tumor resection cavity as a non-nodular, ring-like enhancing structure. Both PP and TN lesions almost exclusively developed in the main prior radiation field. Presence of either condition appeared to be associated with above-average overall survival.
PP and TN occur in clinically distinct patient populations and exhibit differences in spatial radiographic pattern. Increased familiarity with both conditions and their unique features will improve patient management and may avoid unnecessary surgical procedures.
Pseudoprogression (PP) and treatment-induced brain tissue necrosis (TN) are challenging treatment-related effects mimicking tumor progression in patients with brain cancer. Affected patients frequently require surgery to guide management. PP and TN remain arbitrarily defined and insufficiently characterized. Lack of clear diagnostic criteria compromises treatment and may adversely affect outcome interpretation in clinical trials. The present findings in a cohort of patients with glioma with PP/TN suggest that both phenomena exhibit unique clinical and imaging characteristics, manifest in different patient populations, and should be classified as distinct clinical conditions. Increased familiarity with PP and TN key features may guide clinicians toward timely noninvasive diagnosis, circumvent potentially unnecessary surgical procedures, and improve response assessment in neuro-oncology.
假性进展(PP)和治疗引起的脑组织坏死(TN)是具有挑战性的癌症治疗相关效应。这两种现象都没有得到充分的定义;通常需要组织活检才能将其与复发性疾病区分开来。我们在此描述了 PP 和 TN 的独特特征,以促进无创诊断和临床管理。
回顾性比较了经病理证实的胶质瘤患者中表现为放疗(RT)完成后 5 个月内出现的假性进展(PP,定义为<5 个月)或 TN(>5 个月)的临床、影像学和组织病理学数据。每个被诊断为 PP 或 TN 的成像事件/病变(感兴趣区域[ROI])通过连续成像进行纵向评估。
我们共确定了 64 例经活检证实的主要为(80%)PP(n=27)和 TN(n=37)的病例,总共包括 137 个 ROI。PP 和 TN 的中位发病时间分别为 RT 后 1 个月和 11 个月。临床上,PP 更常发生在抗肿瘤治疗的活动期,需要更多的基于类固醇的干预,与胶质母细胞瘤(81%比 40%)、较少的 IDH1 突变和较短的中位总生存期相关。影像学上,TN 病变通常最初表现为脑室周围(n=37;60%),数量更多(中位数,2 个与 1 个 ROI),活检时含有较少的恶性成分。相比之下,PP 主要在肿瘤切除腔周围形成非结节性、环状增强结构。PP 和 TN 病变几乎仅在主要先前放疗野中发展。两种情况下的存在似乎与平均总生存期较高有关。
PP 和 TN 发生在具有临床特征的患者群体中,在空间放射影像学模式上存在差异。提高对这两种情况及其独特特征的认识,将改善患者的管理,并可能避免不必要的手术。
假性进展(PP)和治疗引起的脑组织坏死(TN)是具有挑战性的治疗相关效应,会模仿脑癌患者的肿瘤进展。受影响的患者经常需要手术来指导管理。PP 和 TN 仍然是任意定义的,且特征描述不足。缺乏明确的诊断标准会影响治疗效果,并可能对临床试验的结果解释产生不利影响。本研究在一组经病理证实的脑胶质瘤患者中发现,PP/TN 均具有独特的临床和影像学特征,表现为不同的患者人群,应被归类为不同的临床疾病。增加对 PP 和 TN 主要特征的认识,有助于临床医生进行及时的无创诊断,避免潜在的不必要的手术,并改善神经肿瘤学的反应评估。