Mijic Dragomir, Kurowicki Jennifer, Berglund Derek, Rosas Samuel, McNeely Emmanuel, Motisi Matthew, Polisetty Teja, Levy Jonathan C
Department of Orthopedics, Holy Cross Orthopedic Research Institute, Fort Lauderdale, FL, USA.
Department of Orthopaedic Surgery, Seton Hall University, Nutley, NH, USA.
JSES Int. 2020 Feb 24;4(2):341-346. doi: 10.1016/j.jseint.2019.12.010. eCollection 2020 Jun.
Concomitant biceps tendon pathology is often present in patients undergoing rotator cuff repair (RCR). Management of biceps pathology has been reported to influence outcomes of RCR; however, the impact on the pace of recovery remains unclear. The purpose of this study was to analyze the effects of simultaneous RCR with biceps tenodesis (RCR-BT) on time to achieve maximum improvement and recovery speed for pain and function.
A retrospective review of 535 patients who underwent primary RCR for full-thickness tears. Patients treated with simultaneous RCR-BT were compared with RCR-only. Outcome measures and motion were recorded at preoperative routine postoperative intervals. Plateau in maximal improvement and recovery speed were analyzed for both pain and functional recovery.
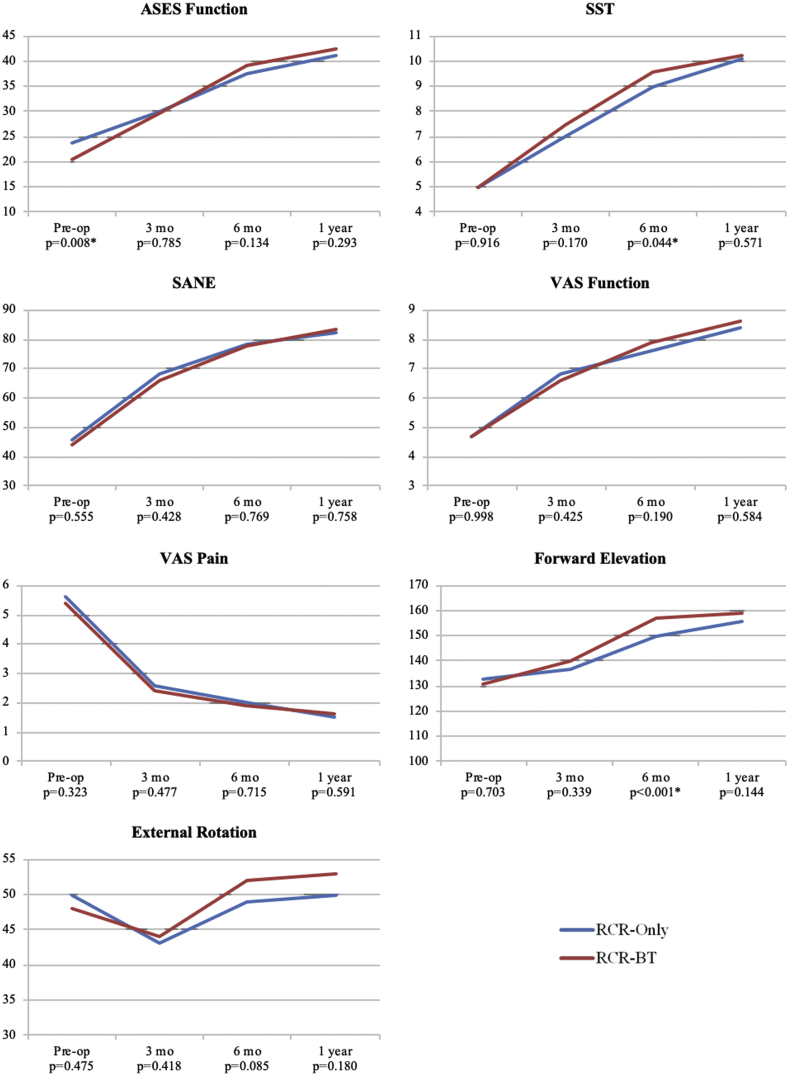
Baseline American Shoulder and Elbow Surgeons Standardized Shoulder Assessment Form (ASES) function was significantly lower for the RCR-BT cohort (20.5) compared with RCR-only (23.9; = .008). For visual analog scale (VAS) pain and measured motion, the plateau in maximal improvement occurred at 6 months for RCR-BT compared with 12 months for the RCR-only group. The remainder of the patient-reported outcome measures took 12 months to achieve a plateau in maximal improvement. At 3 months, 79% of improvement in pain and 42%-49% of functional improvement was achieved in the RCR-BT cohort. Similarly, at 3 months, the RCR-only cohort achieved 73% of pain improvement and 36%-57% of functional improvement at 3 months.
Patients requiring RCR with simultaneous biceps tenodesis have lower baseline ASES function and earlier postoperative plateaus in pain relief and motion improvement following surgery. Nonetheless, the speed of recovery was not influenced by the biceps tenodesis.
肩袖修复术(RCR)患者常伴有肱二头肌肌腱病变。据报道,肱二头肌病变的处理会影响RCR的疗效;然而,其对恢复速度的影响尚不清楚。本研究的目的是分析同期行RCR联合肱二头肌固定术(RCR-BT)对实现疼痛和功能最大改善时间及恢复速度的影响。
回顾性分析535例行全层撕裂初次RCR的患者。将同期行RCR-BT治疗的患者与单纯行RCR的患者进行比较。在术前、术后常规时间间隔记录结果指标和活动情况。分析疼痛和功能恢复的最大改善平台期及恢复速度。
与单纯行RCR的患者(23.9;P = 0.008)相比,RCR-BT组患者的基线美国肩肘外科医师协会标准化肩关节评估表(ASES)功能显著更低(20.5)。对于视觉模拟评分(VAS)疼痛和测量的活动度,RCR-BT组最大改善的平台期出现在术后6个月,而单纯行RCR组为12个月。其余患者报告的结果指标在术后12个月达到最大改善的平台期。在术后3个月时,RCR-BT组实现了79%的疼痛改善和42%-49%的功能改善。同样,在术后3个月时,单纯行RCR组实现了73%的疼痛改善和36%-57%的功能改善。
需要同期行RCR联合肱二头肌固定术的患者基线ASES功能更低,术后疼痛缓解和活动改善的平台期更早。尽管如此,恢复速度不受肱二头肌固定术的影响。