Department of Anesthesiology, First Affiliated Hospital of Anhui Medical University, No.218 Jixi Road, Hefei, 230022, Anhui Province, People's Republic of China.
Department of Anesthesiology, Fuyang Hospital of Anhui Medical University, Fuyang, Anhui Province, People's Republic of China.
BMC Anesthesiol. 2020 Jun 3;20(1):136. doi: 10.1186/s12871-020-01057-z.
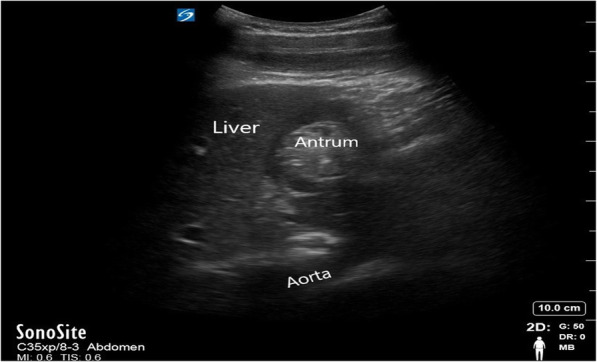
The application of bedside ultrasound to evaluate gastric content and volume can assist in determining aspiration risk. Applying positive pressure ventilation via supraglottic airway devices (SAD) can result in a degree of gastric insufflation. This study assessed and compared the antral cross-sectional area (CSA) in patients undergoing laparoscopic gynecological surgery when managed with different SAD.
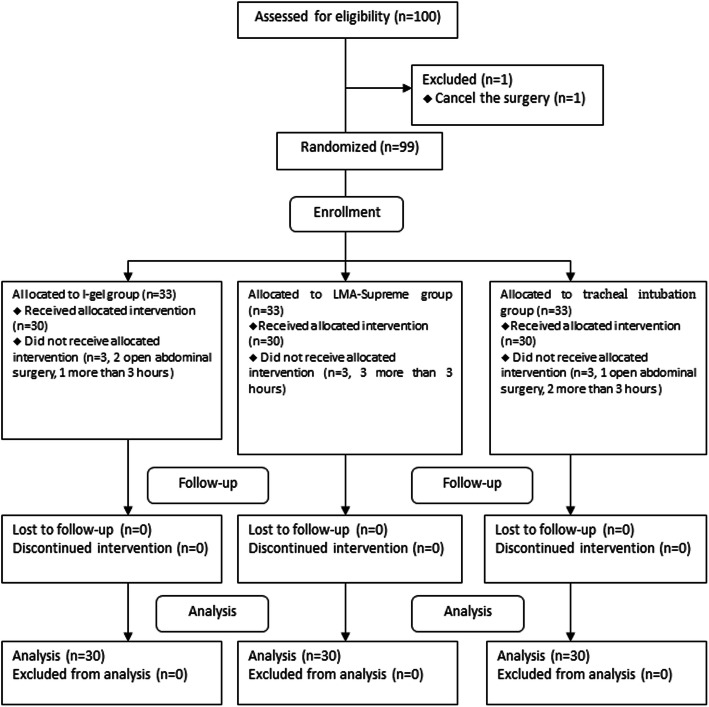
One hundred American Society of Anesthesiologists I or II female patients were assessed for inclusion in this study and divided into three groups of different ventilation devices. Patients were randomly allocated into three groups to receive LMA-Supreme (Group S), I-gel (Group I) or tracheal tube (Group T). The primary outcome was the antral cross-sectional area and secondary outcomes included haemodynamic parameters and postoperative morbidity such as sore throat, hoarseness, dry throat, nausea and vomiting.
The antral CSA was not significantly different among three groups before induction (P = 0.451), after induction (P = 0.456) and at the end of surgery (P = 0.195). The haemodynamic variables were significantly higher in the tracheal tube group than in the LMA-Supreme and I-gel groups after insertion (P < 0.0001) and after removal (P < 0.01). Sore throat was detected in none in the I-gel group compare to two patients (6.7%) in the LMA-Supreme group and fifteen patients (50%) in the tracheal tube group. Hoareness was detected in one (3.3%) in the I-gel group compare to two patients (6.7%) in the LMA-Supreme group and eleven patients (36.7%) in the tracheal tube group.
The SADs do not cause obvious gastric insufflation. Thus, LMA-Supreme and I-gel can be widely used as alternative to endotracheal intubation for the short laparoscopic gynecological surgery.
This trial was registered at the Chinese Clinical Trial Registry (ChiCTR1800018212, data of registration, September 2018).
床边超声应用于评估胃内容物和容量有助于确定误吸风险。使用声门上气道装置(SAD)进行正压通气可导致一定程度的胃充气。本研究评估并比较了接受腹腔镜妇科手术的患者在使用不同 SAD 时的胃窦横截面积(CSA)。
对 100 名美国麻醉医师协会 I 或 II 级女性患者进行评估,纳入本研究,并分为三组不同的通气装置。患者随机分为三组,分别接受 LMA-Supreme(S 组)、I-gel(I 组)或气管导管(T 组)。主要结局是胃窦 CSA,次要结局包括血流动力学参数和术后并发症,如咽痛、声音嘶哑、咽干、恶心和呕吐。
三组患者在诱导前(P=0.451)、诱导后(P=0.456)和手术结束时(P=0.195)的胃窦 CSA 无显著差异。气管导管组的血流动力学变量在插入后(P<0.0001)和取出后(P<0.01)均显著高于 LMA-Supreme 和 I-gel 组。I-gel 组无一例出现咽痛,而 LMA-Supreme 组有 2 例(6.7%),气管导管组有 15 例(50%)。I-gel 组有 1 例(3.3%)出现声音嘶哑,而 LMA-Supreme 组有 2 例(6.7%),气管导管组有 11 例(36.7%)。
SAD 不会引起明显的胃充气。因此,LMA-Supreme 和 I-gel 可广泛用于替代气管内插管进行短时间腹腔镜妇科手术。
本试验在中国临床试验注册中心注册(ChiCTR1800018212,注册数据,2018 年 9 月)。