Department of Anesthesiology, Japan Community Healthcare Organization Tokuyama Central Hospital, Shunan, Japan.
Present address: Department of Anesthesiology and Intensive Care Medicine, Nagoya City University Graduate School of Medical Sciences, Kawasumi 1, Mizuho-cho, Mizuho-ku, Nagoya, Japan.
BMC Anesthesiol. 2021 Jun 28;21(1):181. doi: 10.1186/s12871-021-01406-6.
During laparoscopic gynecological surgery, increased peak airway pressure (PAWP) can cause airway leak upon ventilation with the LMA® ProSeal™. We hypothesized that compared with the use of volume-controlled ventilation (VCV), the use of the AutoFlow® mode would decrease PAWP and airway leak during laparoscopic gynecological surgery with LMA ProSeal.
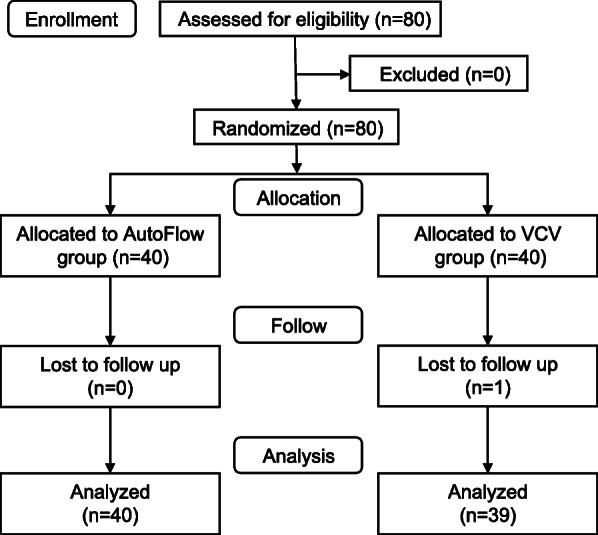
This single-center, randomized, controlled trial allocated 80 adult women undergoing elective laparoscopic gynecological surgery to one of two groups, namely, the AutoFlow group or the VCV group. Ventilation settings for both groups were 8 ml/kg of tidal volume and 5 cmHO of positive end-expiratory pressure, and respiratory rate was adjusted to maintain end-tidal carbon dioxide at 35-40 mmHg. Airway leak, PAWP, and other ventilatory parameters and vital signs were recorded at four timepoints (1, 1 min after insertion of the gastric tube; 2, 2 min after intravenous administration of rocuronium 0.6-0.8 mg/kg; 3, 1 min after initiation of pneumoperitoneum; and 4, 1 min after changing to the Trendelenburg position). The primary outcome was PAWP during pneumoperitoneum and in the Trendelenburg position, whereas the secondary outcomes included PAWP at other timepoints and airway leak development. We used the Mann-Whitney U test for PAWP and Fisher's exact test for comparing airway leak among the groups.
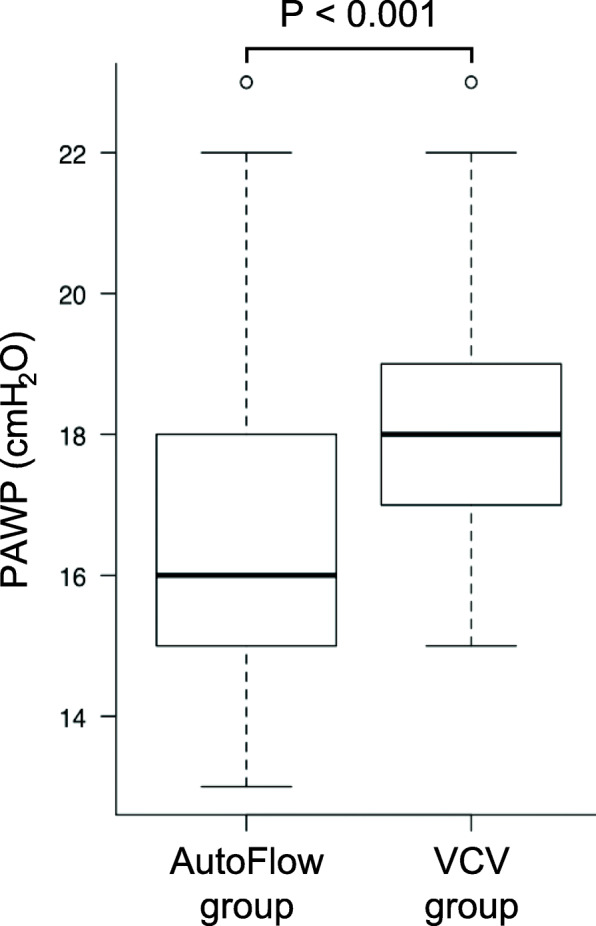
Data from 40 patients in the AutoFlow group and 39 in the VCV group were used for analysis. PAWP at pneumoperitoneum pressure and in the Trendelenburg position was significantly lower in the AutoFlow group than in the VCV group [median (interquartile range), 16 (15-18) cmHO vs. 18 (17-19) cmHO; P < 0.001]. Similarly, patients in the AutoFlow group showed lower PAWP at the other three timepoints measured. Airway leak occurred in four patients in the AutoFlow group and in two patients in the VCV group; however, this incidence was not significantly different (P = 0.68).
Even though AutoFlow ventilation decreased PAWP, it did not reduce the incidence of airway leak compared with VCV during laparoscopic gynecological surgery with the LMA ProSeal.
UMIN Clinical Trials Registry, identifier UMIN000023173 .
在腹腔镜妇科手术中,使用 LMA® ProSeal™ 进行通气时,气道峰压(PAWP)升高可导致气道泄漏。我们假设与使用容量控制通气(VCV)相比,使用 AutoFlow®模式可降低 LMA ProSeal 腹腔镜妇科手术中的 PAWP 和气道泄漏。
这是一项单中心、随机、对照试验,将 80 名择期行腹腔镜妇科手术的成年女性随机分配至 AutoFlow 组或 VCV 组。两组的通气设置均为 8ml/kg 的潮气量和 5cmH2O 的呼气末正压,呼吸频率调整以维持呼气末二氧化碳在 35-40mmHg。在四个时间点(1:胃管插入后 1 分钟;2:静脉注射罗库溴铵 0.6-0.8mg/kg 后 2 分钟;3:气腹开始后 1 分钟;4:改为头高脚低位后 1 分钟)记录气道泄漏、PAWP 及其他通气参数和生命体征。主要结局为气腹和头高脚低位时的 PAWP,次要结局包括其他时间点的 PAWP 和气道泄漏的发展。我们使用 Mann-Whitney U 检验比较 PAWP,使用 Fisher 确切检验比较组间气道泄漏。
AutoFlow 组和 VCV 组各有 40 例和 39 例患者的数据用于分析。AutoFlow 组气腹压和头高脚低位时的 PAWP 明显低于 VCV 组[中位数(四分位距),16(15-18)cmH2O 比 18(17-19)cmH2O;P<0.001]。同样,AutoFlow 组在其余三个测量时间点的 PAWP 也较低。AutoFlow 组有 4 例患者发生气道泄漏,VCV 组有 2 例患者发生气道泄漏,但发生率无显著差异(P=0.68)。
即使 AutoFlow 通气降低了 PAWP,但与 LMA ProSeal 腹腔镜妇科手术中的 VCV 相比,并未降低气道泄漏的发生率。
UMIN 临床研究注册,注册号 UMIN000023173。