Department of Anesthesiology, University of Virginia, Charlottesville, Virginia, United States of America.
Department of Neurological Surgery, University of Virginia, Charlottesville, Virginia, United States of America.
PLoS One. 2020 Jun 4;15(6):e0234199. doi: 10.1371/journal.pone.0234199. eCollection 2020.
To mitigate the recent nationwide shortage of intravenous opioids, we developed a standardized perioperative oral opioid guideline anchored with appropriate use of nonopioid analgesia, neuraxial and loco-regional techniques. We hypothesize that adoption of this new guideline was associated with: 1) equivalent patient reported pain scores in the post-anesthesia care unit (PACU); and 2) equivalent total opioid use (oral and parenteral) during the perioperative period.
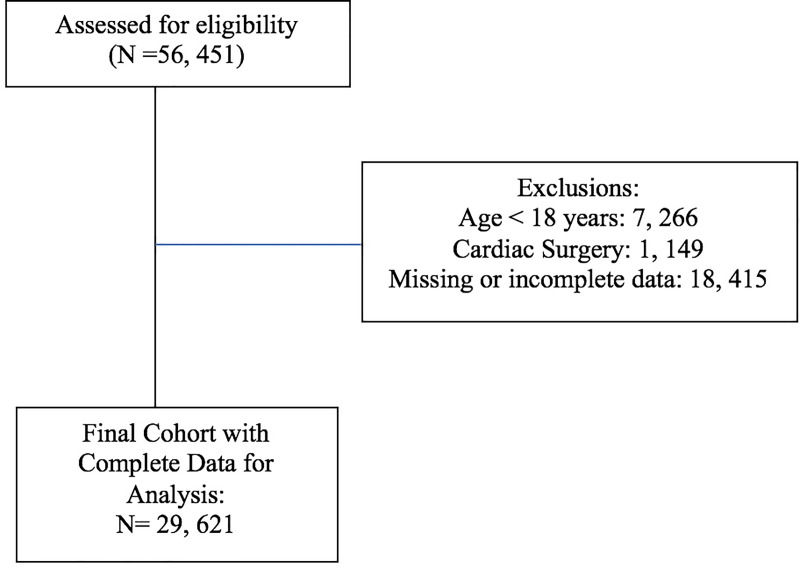
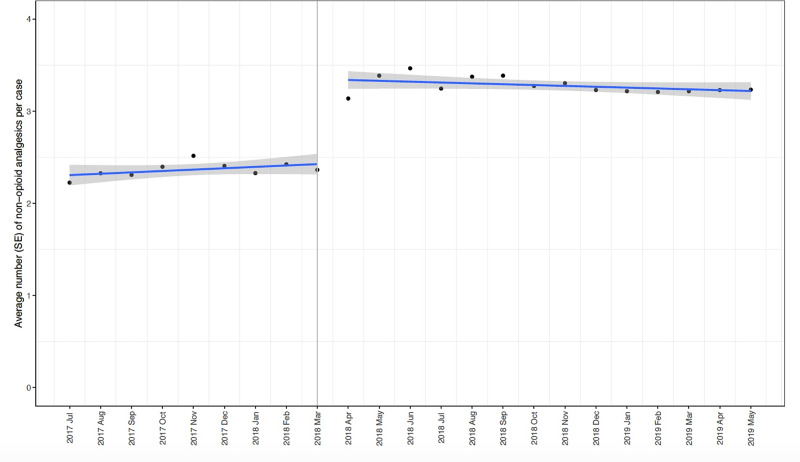
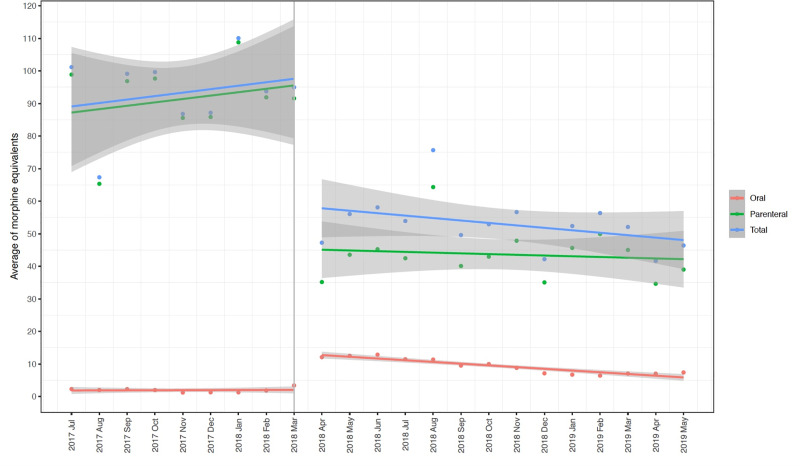
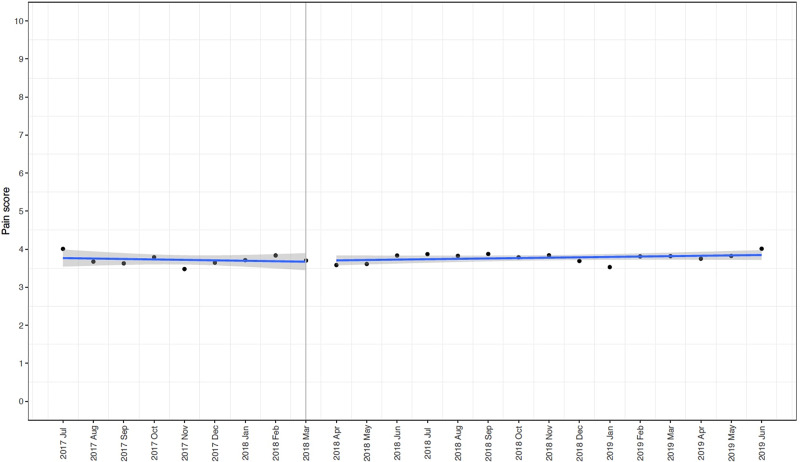
Cases performed from July 1, 2017 to May 31, 2019 were screened. All opioids administered were converted to intravenous morphine milligram equivalents. Segmented regression analyses of interrupted time series were performed examining the change in opioid use, PACU pain scores and number of non-opioid analgesic medications used before and after the protocol implementation in April 2018.
After exclusions, 29, 621 cases were included in the analysis. No significant differences in demographic, ASA status, case length and surgical procedure type were present in the pre and post-intervention period. A significant decrease in total (Estimate: -39.9 mg, SE: 6.9 mg, p < 0.001) and parenteral (Estimate: -51.6 mg, SE: 7.1 mg, p < 0.001) opioid use with a significant increase in oral opioid use (Estimate: 9.4 mg, SE: 1.1 mg, p < 0.001) was noted after the intervention. Pain scores were not significantly different between the pre- and post-intervention period (Estimate: 0.05, SE: 0.13, p = 0.69).
We report our experience with a primary perioperative oral based opioid regimen that is associated with decreased total opioid consumption and equivalent patient reported pain scores.
为缓解近期全国范围内静脉阿片类药物短缺的问题,我们制定了一个标准化的围手术期口服阿片类药物指南,该指南以适当使用非阿片类镇痛、椎管内和局部区域技术为基础。我们假设采用这种新的指南与以下两点有关:1)患者在麻醉后护理单元(PACU)报告的疼痛评分相当;2)围手术期内口服和静脉使用的总阿片类药物量相当。
筛选了 2017 年 7 月 1 日至 2019 年 5 月 31 日期间进行的病例。所有给予的阿片类药物均转换为静脉用吗啡毫克当量。在 2018 年 4 月实施方案前后,采用分段回归分析中断时间序列,观察阿片类药物使用量、PACU 疼痛评分和非阿片类镇痛药物使用数量的变化。
排除后,共纳入 29621 例病例进行分析。在干预前后的预干预和后干预期间,在人口统计学、ASA 状态、病例长度和手术类型方面没有显著差异。总(估计值:-39.9 毫克,SE:6.9 毫克,p<0.001)和静脉(估计值:-51.6 毫克,SE:7.1 毫克,p<0.001)阿片类药物用量显著减少,而口服阿片类药物用量显著增加(估计值:9.4 毫克,SE:1.1 毫克,p<0.001)。干预后疼痛评分在预干预和后干预期间无显著差异(估计值:0.05,SE:0.13,p=0.69)。
我们报告了一种主要的围手术期口服阿片类药物方案的经验,该方案与总阿片类药物消耗减少和患者报告的疼痛评分相当。