Department of Dermatology, Columbia University Irving Medical Center, New York, New York, USA.
Department of Pathology and Cell Biology, Division of Renal Pathology, Columbia University Irving Medical Center, New York, New York, USA.
J Immunother Cancer. 2020 Jun;8(1). doi: 10.1136/jitc-2020-000908.
Immune checkpoint blockade has emerged as a highly effective treatment for patients with metastatic melanoma and cutaneous squamous cell carcinoma. Nivolumab blocks the interactions between programmed cell death protein 1 and programmed death ligand 1 allowing for activation of a latent immune response against the malignancy. Ipilimumab binds to and blocks cytotoxic T-lymphocyte-associated protein 4, alleviating the negative regulation of T-cell activation that is mediated by that checkpoint. Combination therapy with nivolumab and ipilimumab is associated with longer overall survival at 5 years compared with nivolumab monotherapy. Solid organ transplant recipients have a significantly higher risk of malignancies compared with the general population. There is limited data surrounding the efficacy of combination immunotherapy in solid organ transplant recipients, as these patients were excluded from seminal trials due to risk of organ rejection.
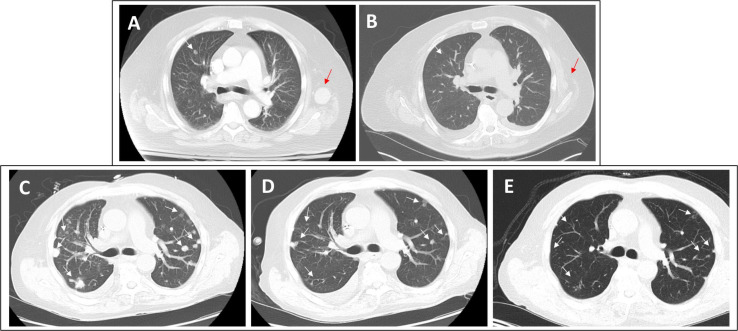
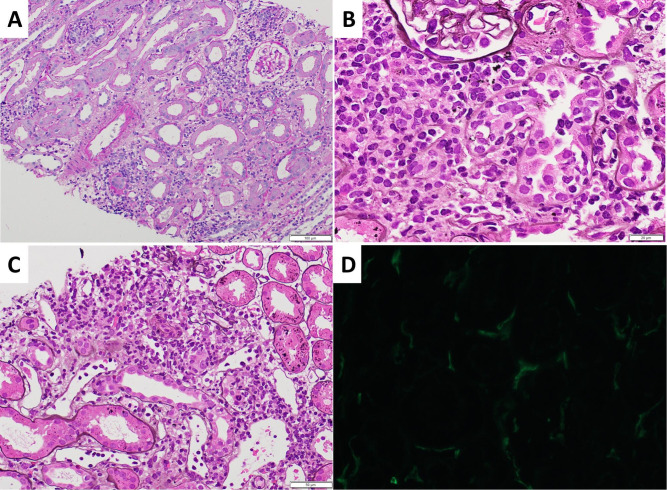
Here we present four cases of combination immunotherapy in kidney transplant recipients. Three patients had metastatic melanoma, and one patient had metastatic cutaneous squamous cell carcinoma. Two patients had radiographic responses from immunotherapy, one patient had stable disease, and one patient had disease progression. Only one patient had biopsy-proven rejection. At last follow-up, three patients had functioning grafts, though one required hemodialysis after treatment, and one patient succumbed to disease, but graft function remained intact throughout her course.
These cases describe the use of ipilimumab and nivolumab combination immunotherapy for cutaneous malignancies in kidney transplant recipients. They highlight the potential to preserve kidney graft function while effectively treating the disease.
NCT03816332.
免疫检查点阻断已成为治疗转移性黑色素瘤和皮肤鳞状细胞癌患者的一种非常有效的方法。Nivolumab 阻断程序性细胞死亡蛋白 1 和程序性死亡配体 1 之间的相互作用,从而激活针对恶性肿瘤的潜在免疫反应。Ipilimumab 与细胞毒性 T 淋巴细胞相关蛋白 4 结合并阻断其功能,从而减轻由该检查点介导的 T 细胞活化的负调节。与 nivolumab 单药治疗相比,nivolumab 和 ipilimumab 的联合治疗可使患者的总生存期在 5 年内延长。与普通人群相比,实体器官移植受者发生恶性肿瘤的风险显著更高。由于存在器官排斥的风险,这些患者被排除在主要试验之外,因此关于实体器官移植受者联合免疫治疗疗效的数据有限。
本文报告了 4 例肾移植受者接受联合免疫治疗的病例。3 例患者患有转移性黑色素瘤,1 例患者患有转移性皮肤鳞状细胞癌。2 例患者的免疫治疗有影像学反应,1 例患者病情稳定,1 例患者疾病进展。只有 1 例患者经活检证实有排斥反应。最后一次随访时,3 例患者的移植物功能正常,尽管其中 1 例在治疗后需要血液透析,1 例患者死于疾病,但整个病程中移植物功能保持完整。
这些病例描述了在肾移植受者中使用 ipilimumab 和 nivolumab 联合免疫疗法治疗皮肤恶性肿瘤。它们强调了在有效治疗疾病的同时保留肾移植功能的潜力。
NCT03816332。