Dept. of Neurology, Clinical Neuroscience Center, University Hospital Zurich and University of Zurich, Frauenklinikstrasse 26, 8091, Zurich, Switzerland.
Dept. of Neurosurgery, Clinical Neuroscience Center, University Hospital Zurich and University of Zurich, Zürich, Switzerland.
Transl Stroke Res. 2021 Feb;12(1):39-48. doi: 10.1007/s12975-020-00821-0. Epub 2020 Jun 6.
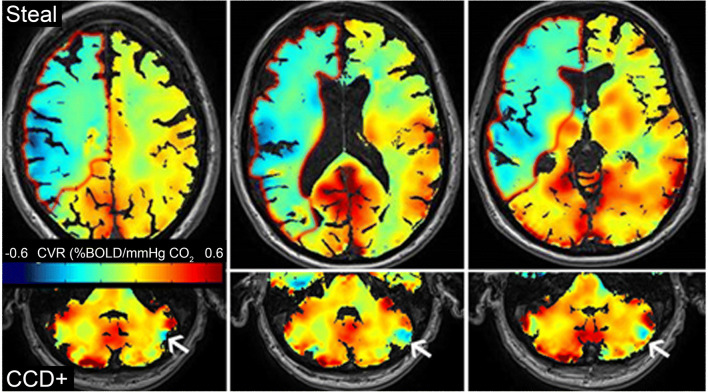
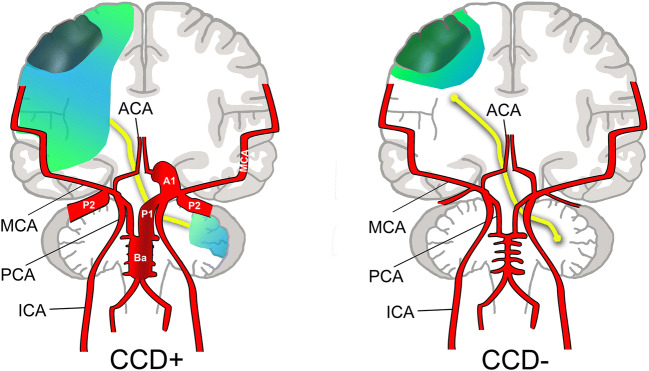
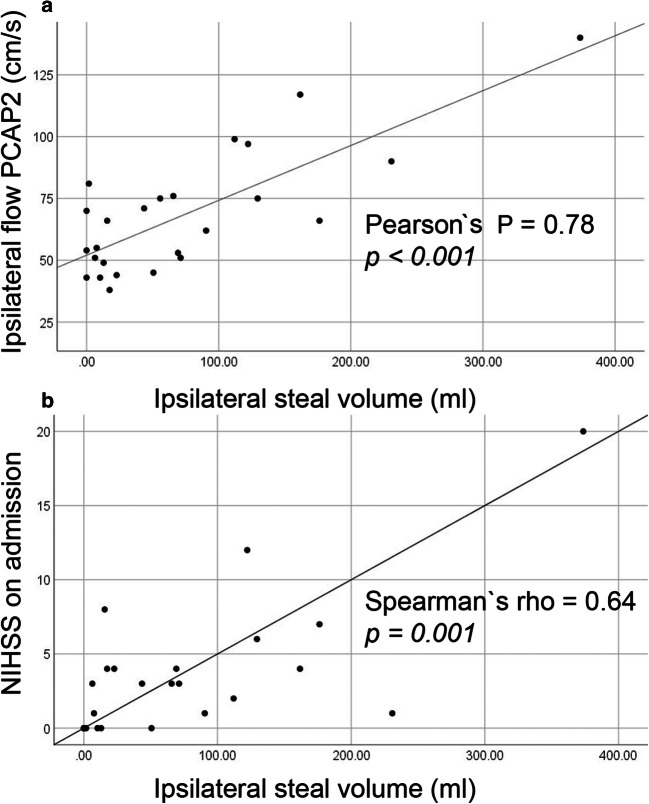
Crossed cerebellar diaschisis (CCD) in internal carotid artery (ICA) stroke refers to attenuated blood flow and energy metabolism in the contralateral cerebellar hemisphere. CCD is associated with an interruption of cerebro-cerebellar tracts, but the precise mechanism is unknown. We hypothesized that in patients with ICA occlusions, CCD might indicate severe hemodynamic impairment in addition to tissue damage. Duplex sonography and clinical data from stroke patients with unilateral ICAO who underwent blood oxygen-level-dependent MRI cerebrovascular reserve (BOLD-CVR) assessment were analysed. The presence of CCD (either CCD+ or CCD-) was inferred from BOLD-CVR. We considered regions with negative BOLD-CVR signal as areas suffering from hemodynamic steal. Twenty-five patients were included (11 CCD+ and 14 CCD-). Stroke deficits on admission and at 3 months were more severe in the CCD+ group. While infarct volumes were similar, CCD+ patients had markedly larger BOLD steal volumes than CCD- patients (median [IQR] 122.2 [111] vs. 11.6 [50.6] ml; p < 0.001). Furthermore, duplex revealed higher peak-systolic flow velocities in the intracranial collateral pathways. Strikingly, posterior cerebral artery (PCA)-P2 velocities strongly correlated with the National Institute of Health Stroke Scale on admission and BOLD-CVR steal volume. In patients with strokes due to ICAO, the presence of CCD indicated hemodynamic impairment with larger BOLD-defined steal volume and higher flow in the ACA/PCA collateral system. Our data support the concept of a vascular component of CCD as an indicator of hemodynamic failure in patients with ICAO.
大脑交叉失联络(CCD)是指颈内动脉(ICA)卒中患者对侧小脑半球的血流和能量代谢减弱。CCD 与脑-小脑束中断有关,但确切机制尚不清楚。我们假设在 ICA 闭塞的患者中,CCD 可能除了组织损伤外,还提示严重的血流动力学障碍。对接受血氧水平依赖磁共振脑血管储备(BOLD-CVR)评估的单侧 ICAO 卒中患者的超声双功和临床数据进行分析。通过 BOLD-CVR 推断 CCD(CCD+或 CCD-)的存在。我们认为负 BOLD-CVR 信号的区域为存在血流动力学盗血的区域。共纳入 25 例患者(11 例 CCD+和 14 例 CCD-)。CCD+组患者入院和 3 个月时的卒中缺损更严重。尽管梗死体积相似,但 CCD+患者的 BOLD 盗血体积明显大于 CCD-患者(中位数[四分位距] 122.2[111]ml 比 11.6[50.6]ml;p<0.001)。此外,超声双功显示颅内侧支循环的收缩期峰值流速更高。引人注目的是,大脑后动脉(PCA)-P2 流速与入院时的国立卫生研究院卒中量表(NIHSS)和 BOLD-CVR 盗血体积强烈相关。在 ICAO 导致的卒中患者中,CCD 的存在表明存在血流动力学障碍,BOLD 定义的盗血体积较大,ACA/PCA 侧支循环系统的血流较高。我们的数据支持 CCD 作为 ICAO 患者血流动力学衰竭的血管成分的概念。