van Niftrik Christiaan H B, Visser Thomas F, Sebök Martina, Muscas Giovanni, El Amki Mohamad, Serra Carlo, Regli Luca, Wegener Susanne, Fierstra Jorn
Department of Neurosurgery, University Hospital Zurich, University of Zurich, 8091 Zurich, Switzerland.
Clinical Neuroscience Center, University Hospital Zurich, University of Zurich, 8091 Zurich, Switzerland.
Brain Commun. 2021 Nov 24;3(4):fcab279. doi: 10.1093/braincomms/fcab279. eCollection 2021.
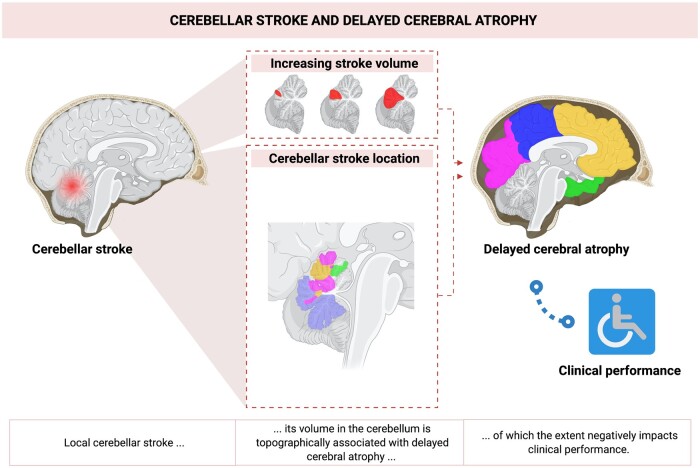
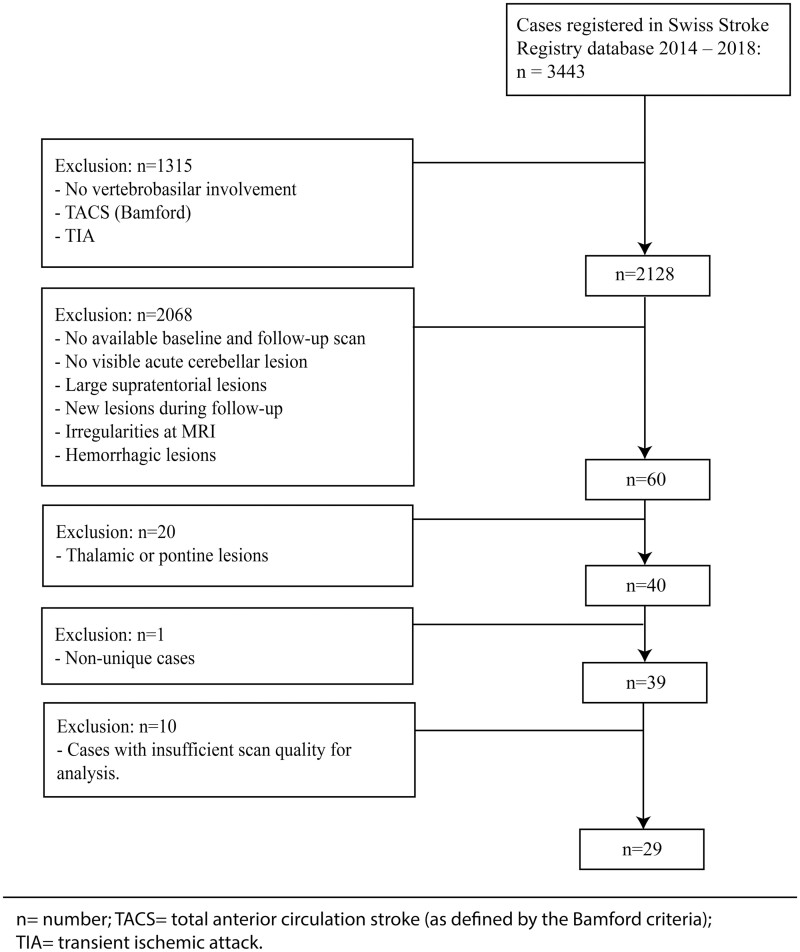
Remote dysconnectivity following cerebellar ischaemic stroke may have a negative impact on supratentorial brain tissue. Since the cerebellum is connected to the individual cerebral lobes via contralateral tracts, cerebellar lesion topography might determine the distribution of contralateral supratentorial brain tissue changes. We investigated (i) the occurrence of delayed cerebral atrophy after cerebellar ischaemic stroke and its relationship to infarct volume; (ii) whether cerebellar stroke topography determines supratentorial atrophy location; and (iii) how cortical atrophy after cerebellar stroke impacts clinical outcome. We performed longitudinal volumetric MRI analysis of patients with isolated cerebellar stroke from the Swiss Stroke Registry database. Stroke location and volume were determined at baseline MRI. Delayed cerebral atrophy was measured as supratentorial cortical volumetric change at follow-up, in contralateral target as compared to ipsilateral reference-areas. In patients with bilateral stroke, both hemispheres were analysed separately. We obtained maps of how cerebellar lesion topography, determines the probability of delayed atrophy per distinct cerebral lobe. Clinical performance was measured with the National Institutes of Health Stroke Scale and modified Rankin Scale. In 29 patients (age 58 ± 18; 9 females; median follow-up: 6.2 months), with 36 datasets (7 patients with bilateral cerebellar stroke), delayed cerebral atrophy occurred in 28 (78%) datasets. A multivariable generalized linear model for a Poisson distribution showed that infarct volume (milliliter) in bilateral stroke patients was positively associated with the number of atrophic target areas (Rate ratio = 1.08; = 0.01). Lobe-specific cerebral atrophy related to distinct topographical cerebellar stroke patterns. By ordinal logistic regression (shift analysis), more atrophic areas predicted higher 3-month mRS scores in patients with low baseline scores (baseline score 3-5: Odds ratio = 1.34; = 0.02; baseline score 0-2: OR = 0.71; = 0.19). Our results indicate that (i) isolated cerebellar ischaemic stroke commonly results in delayed cerebral atrophy and stroke volume determines the severity of cerebral atrophy in patients with bilateral stroke; (ii) cerebellar stroke topography affects the location of delayed cerebral atrophy; and (iii) delayed cerebral atrophy negatively impacts clinical outcome.
小脑缺血性中风后的远程失连接可能会对幕上脑组织产生负面影响。由于小脑通过对侧传导束与各个脑叶相连,小脑病变的部位可能决定对侧幕上脑组织变化的分布。我们调查了:(i)小脑缺血性中风后迟发性脑萎缩的发生情况及其与梗死体积的关系;(ii)小脑中风部位是否决定幕上萎缩的位置;以及(iii)小脑中风后的皮质萎缩如何影响临床结局。我们对来自瑞士中风登记数据库的孤立性小脑中风患者进行了纵向容积MRI分析。在基线MRI时确定中风部位和体积。迟发性脑萎缩通过随访时幕上皮质容积变化来测量,与同侧参考区域相比,测量对侧目标区域的变化。对于双侧中风患者,分别分析两个半球。我们获得了小脑病变部位如何决定每个不同脑叶迟发性萎缩概率的图谱。临床表现在国立卫生研究院卒中量表和改良Rankin量表上进行测量。在29例患者(年龄58±18岁;9名女性;中位随访时间:6.2个月)中,有36个数据集(7例双侧小脑中风患者),28个(78%)数据集出现了迟发性脑萎缩。一个用于泊松分布的多变量广义线性模型显示,双侧中风患者的梗死体积(毫升)与萎缩目标区域的数量呈正相关(率比=1.08; =0.01)。特定脑叶的脑萎缩与不同的小脑中风部位模式相关。通过有序逻辑回归(移位分析),在基线评分较低的患者中,更多的萎缩区域预测3个月时改良Rankin量表评分更高(基线评分3 - 5分:优势比=1.34; =0.02;基线评分0 - 2分:优势比=0.71; =0.19)。我们的结果表明:(i)孤立性小脑缺血性中风通常会导致迟发性脑萎缩,中风体积决定了双侧中风患者脑萎缩的严重程度;(ii)小脑中风部位影响迟发性脑萎缩的位置;以及(iii)迟发性脑萎缩对临床结局有负面影响。