Department of Neurosurgery, Medical Center - University of Freiburg, Faculty of Medicine, University of Freiburg, Breisacher Str. 64, 79106, Freiburg, Germany.
Department of Neurosurgery, Universitair Ziekenhuis Brussel, VUB University, Brussels, Belgium.
Childs Nerv Syst. 2020 Oct;36(10):2537-2552. doi: 10.1007/s00381-020-04712-5. Epub 2020 Jun 7.
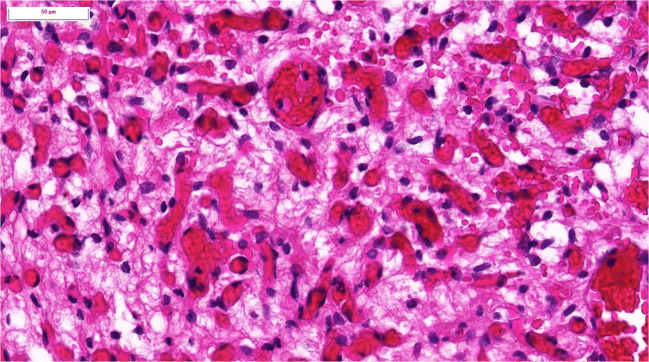
Hemangioblastomas are rare, histologically benign, highly vascularized tumors of the brain, the spinal cord, and the retina, occurring sporadically or associated with the autosomal dominant inherited von Hippel-Lindau (VHL) disease. Children or adults with VHL disease have one of > 300 known germline mutations of the VHL gene located on chromosome 3. They are prone to develop hemangioblastomas, extremely rarely starting at age 6, rarely at age 12-18, and, typically and almost all, as adults. There is a plethora of VHL-associated tumors and cysts, mainly in the kidney, pancreas, adrenals, reproductive organs, and central nervous system. Due to a lack of causal treatment, alleviation of symptoms and prevention of permanent neurological deficits as well as malignant transformation are the main task. Paucity of data and the nonlinear course of tumor progression make management of pediatric VHL patients with hemangioblastomas challenging.
The Freiburg surveillance protocol was developed by combining data from the literature and our experience of examinations of > 300 VHL patients per year at our university VHL center.
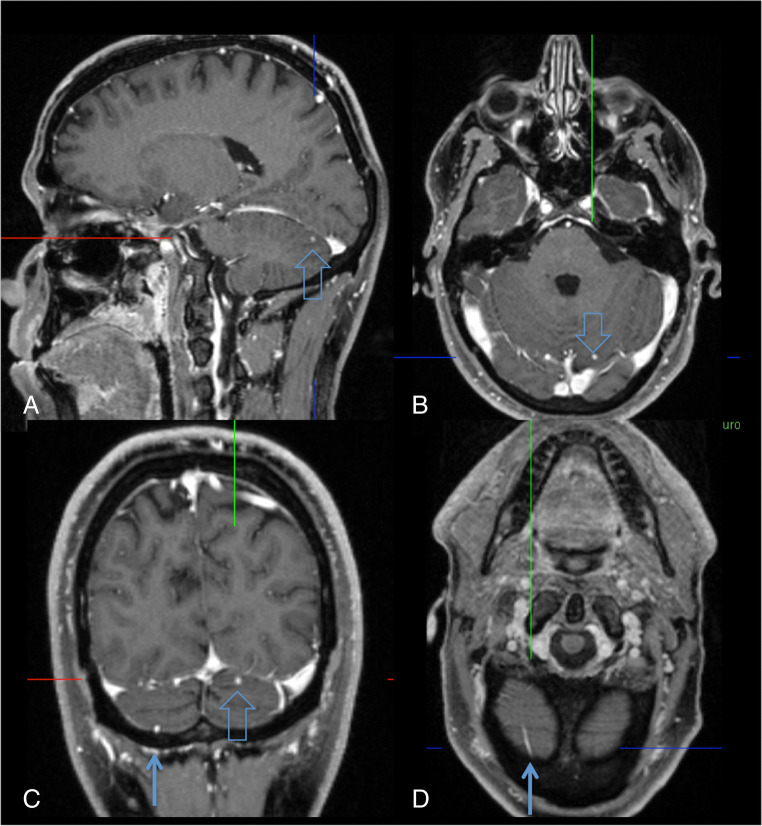
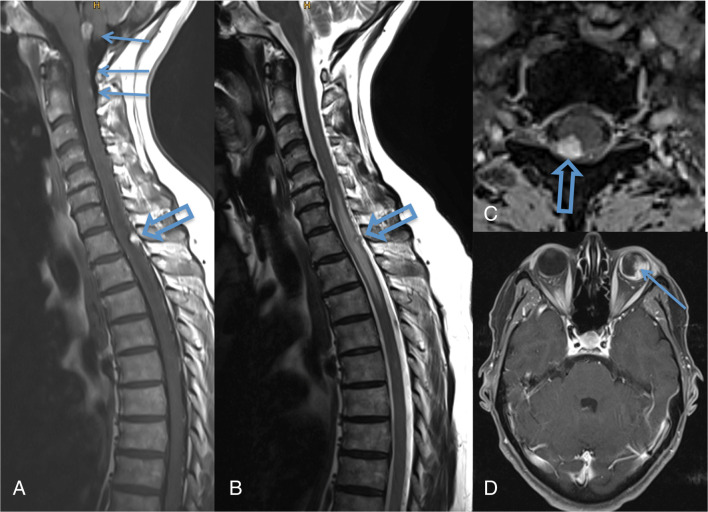
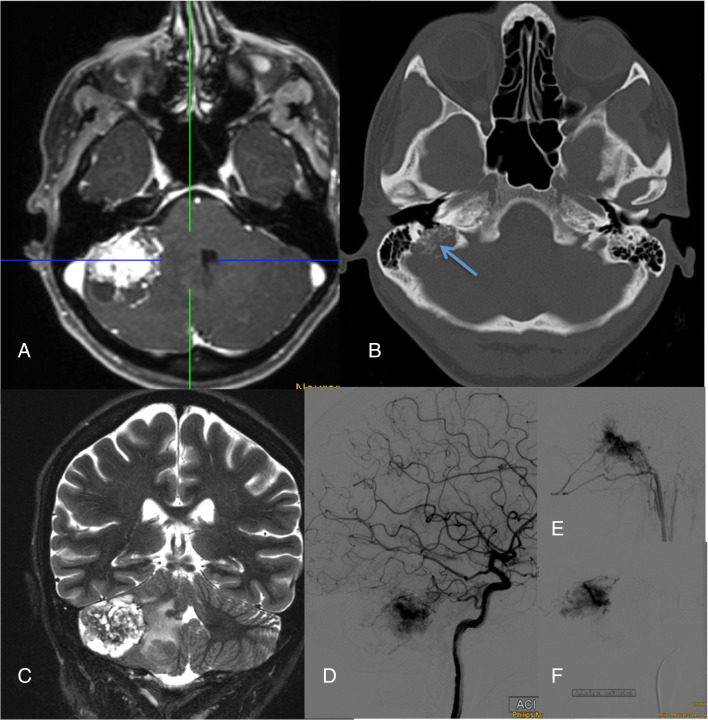
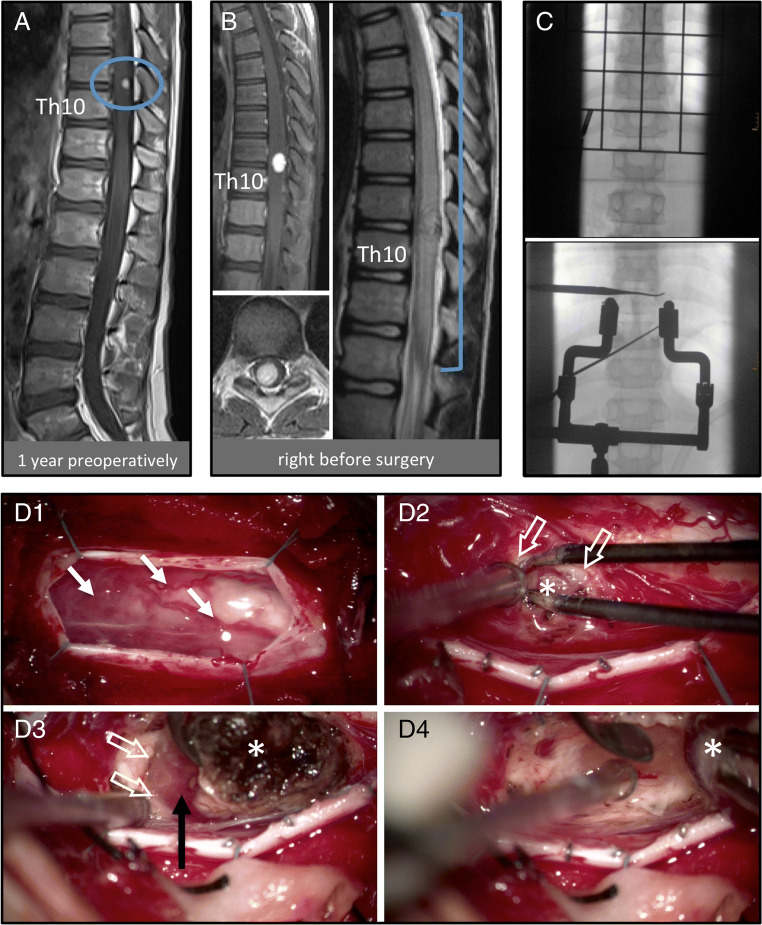
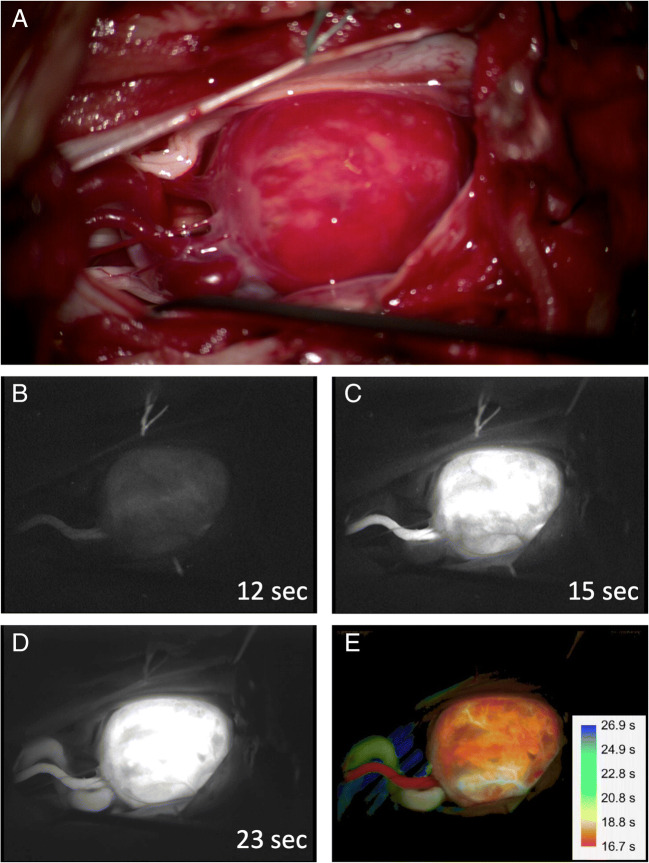
Key recommendations are to start screening of patients at risk by funduscopy with dilated pupils for retinal tumors with admission to school and with MRI of the brain and spinal cord at age 14, then continue biannually until age 18, with emergency MRI in case of neurological symptoms. Indication for surgery remains personalized and should be approved by an experienced VHL board, but we regard neurological symptoms, rapid tumor growth, or critically large tumor/cyst sizes as the key indications to remove hemangioblastomas. Since repeated surgery on hemangioblastomas in VHL patients is not rare, modern neurosurgical techniques should encompass microsurgery, neuronavigation, intraoperative neuromonitoring, fluorescein dye-based intraoperative angiography, intraoperative ultrasound, and minimally invasive approaches, preceded in selected cases by endovascular embolization. Highly specialized neurosurgeons are able to achieve a very low risk of permanent morbidity for the removal of hemangioblastomas from the cerebellum and spinal cord. Small retinal tumors of the peripheral retina can be treated by laser coagulation, larger tumors by cryocoagulation or brachytherapy.
We consider management at experienced VHL centers mandatory and careful surveillance and monitoring of asymptomatic lesions are required to prevent unnecessary operations and minimize morbidity.
血管母细胞瘤是一种罕见的、组织学良性的、高度血管化的脑、脊髓和视网膜肿瘤,可散发或与常染色体显性遗传的 von Hippel-Lindau(VHL)病相关。患有 VHL 病的儿童或成人有超过 300 种已知的 VHL 基因突变,这些突变位于 3 号染色体上。他们容易发生血管母细胞瘤,极少数在 6 岁时开始发病,极少数在 12-18 岁时发病,通常且几乎所有患者均在成年时发病。VHL 还会导致多种相关的肿瘤和囊肿,主要位于肾脏、胰腺、肾上腺、生殖器官和中枢神经系统。由于缺乏因果治疗,缓解症状和预防永久性神经功能缺损以及恶性转化是主要任务。由于缺乏数据以及肿瘤进展的非线性,管理患有血管母细胞瘤的儿科 VHL 患者具有挑战性。
弗莱堡监测方案是通过结合文献数据和我们在大学 VHL 中心每年对 300 多名 VHL 患者的检查经验而制定的。
关键建议是通过瞳孔扩张的眼底检查开始对有风险的患者进行视网膜肿瘤筛查,在入学时开始,并在 14 岁时进行脑和脊髓 MRI 检查,然后每两年进行一次检查,直到 18 岁,如果出现神经症状则进行紧急 MRI。手术指征仍然是个体化的,应由经验丰富的 VHL 委员会批准,但我们认为神经症状、肿瘤快速生长或临界大的肿瘤/囊肿大小是切除血管母细胞瘤的关键指征。由于 VHL 患者的血管母细胞瘤反复手术并不罕见,因此现代神经外科技术应包括显微外科手术、神经导航、术中神经监测、荧光素染料术中血管造影、术中超声和微创方法,并在选择性病例中进行血管内栓塞。经验丰富的神经外科医生能够非常低的风险为小脑和脊髓的血管母细胞瘤切除而获得永久性发病率。周边视网膜的小视网膜肿瘤可以通过激光凝固治疗,较大的肿瘤可以通过冷冻治疗或近距离放射治疗。
我们认为在有经验的 VHL 中心进行管理是强制性的,需要对无症状病变进行仔细的监测和监测,以防止不必要的手术并将发病率降至最低。